
- GmarShops Marketplace , Air Jordan 1 Retro Low Og Neutral Grey , Jordan 12 Field Purple
- Melania Trump's Hands on Donald's Trip Make a Subtle Style Statement
- Taylor Swift & Sabrina Carpenter's Height Contrasts at AMAs Go Viral
- TGKB5 ✦ Одяг, Взуття, Аксесуари, Товари для дому, Електроніка та Косметика для жінок та чоловіків
- Jordan 1 Low SB - Practice Team - Maryland football DT Jordan Phillips makes Shrine Bowl All
- Air Jordan 1 Electro Orange 555088 180
- sacai nike ldwaffle white wolf BV0073 100 on feet release date
- Air Jordan 4 DIY Kids DC4101 100 Release Date 4
- air jordan 1 retro high og university blue 555088 134
- nike kyrie 7 expressions dc0589 003 release date info
- Home
- Articles Archive, 2006-2016
- Golden Oldies
- 2016-2025 Articles Archive
- About This Site
- As Relevant Now as It Was One Hundred Six Years Ago: Our Lady's Fatima Message
- Donations (February 10, 2025)
- Now Available for Purchase: Paperback Edition of G.I.R.M. Warfare: The Conciliar Church's Unremitting Warfare Against Catholic Faith and Worship
- Ordering Dr. Droleskey's Books
Revised and Expanded: Sin: More Deadly Than the Coronavirus, part twenty
A global genocide has been taking place since the weaponized SARS-CoV-2 Coronavirus leaked from the Wuhan Institute of Virology in December of 2019.
I. Standardization of Improper Medical Protocols
The first part of this genocide involved the standardization of improper medical protocols to subject everyone who contracted the virus to the same treatment regardless of age or condition. Patients were treated on a cookie-cutter, one-size-fits-all as a series of “guidelines” developed by the Centers for Disease Control and Dr, Anthony Fauci’s National Institute for Allergies and Infectious Diseases denied patients access to such treatments as Ivermectin, Hydroxychlorquine, and massive doses of Vitamins C, D, and Zinc. A disease that is not fatal to most people unless they are elderly or have underlying medical conditions that compromise their immune systems became the means by which fascistic “healthcare experts,” unelected government apparatchiks, many of whom had ties to the Chinese Communist Party in one way or another, and elected officials intent on repressing dissent became a political weapon to be employed on unsuspecting patients as an unstated part of the World Health Organization’s and World Economic Forums “global reset.” The very people who have been using contraception and abortion to depopulate Europe and to have used vaccines to sterilize many women in Third World countries seized an opportunity to kill off “useless eaters” and to govern in a totalitarian manner in the name of “public health” and “global security.” As I noted in part one of this series nearly three years ago, the coronavirus plandemic has been and continues to be about social control, not public health.
The government of the United States of America under the fearlessly intrepid shooter down of science projects, one which was shot down over western Alaska on Saturday, February 11, 2023, at the exact time that the Northern Illinois Bottlecap Balloon Brigade (NIBBB) lost track of their balloon over the same area (see Illinois hobby club fears its balloon was shot down by the USAF; NORAD responds), has become a signatory to an agreement that would give the Red Chinese vassal known as the World Health Organization complete sovereignty over American public health policies during a pandemic.
The Biden administration is preparing to sign up the United States to a ‘legally binding’ accord with the World Health Organization (WHO) that would give this Geneva-based UN subsidiary the authority to dictate America’s policies during a pandemic.
Despite widespread criticism of the WHO’s response to the COVID pandemic, U.S. Health and Human Services (HHS) Secretary Xavier Becerra joined with WHO Director-General Tedros Adhanom Ghebreyesus in September 2022 to announce ‘the U.S.-WHO Strategic Dialogue.’ Together, they developed a ‘platform to maximize the longstanding U.S. government-WHO partnership, and to protect and promote the health of all people around the globe, including the American people.’
These discussions and others spawned the ‘zero draft’ of a pandemic treaty, published on Feb. 1, which now seeks ratification by all 194 WHO member states. A meeting of the WHO’s Intergovernmental Negotiating Body (INB) is scheduled for Feb. 27 to work out the final terms, which all members will then sign.
Written under the banner of ‘the world together equitably,’ the zero draft grants the WHO the power to declare and manage a global pandemic emergency. Once a health emergency is declared, all signatories, including the United States, would submit to the authority of the WHO regarding treatments, government regulations such as lockdowns and vaccine mandates, global supply chains, and monitoring and surveillance of populations.
The WHO pandemic treaty is part of a two-track effort, coinciding with an initiative by the World Health Assembly (WHA) to create new global pandemic regulations that would also supersede the laws of member states. The WHA is the rule-making body of the WHO, comprised of representatives from the member states.
‘Both [initiatives] are fatally dangerous,’ Francis Boyle, professor of international law at Illinois University, told The Epoch Times. ‘Either one or both would set up a worldwide medical police state under the control of the WHO, and in particular WHO Director-General Tedros. If either one or both of these go through, Tedros or his successor will be able to issue orders that will go all the way down the pipe to your primary care physicians.’ A key question surrounding the accord is whether the Biden administration can bind America to treaties and agreements without the consent of the U.S. Senate, which is required under the Constitution. The zero draft concedes that, per international law, treaties between countries must be ratified by national legislatures, thus respecting the right of their citizens to consent. However, the draft also includes a clause that the accord will go into effect on a ‘provisional’ basis, as soon as it is signed by delegates to the WHO, and therefore it will be legally binding on members without being ratified by legislatures. There are several U.S. Supreme Court decisions that may support the Biden administration in this. They include State of Missouri v. Holland, in which the Supreme Court ruled that treaties supersede state laws. Other decisions, such as United States v. Belmont, ruled that executive agreements without Senate consent can be legally binding, with the force of treaties. The WHO, the U.S. Health and Human Services Department, and the World Bank were contacted regarding this article but did not provide a response. Assuming the Regime finalizes this agreement, our liberties will completely evaporate when the next pandemic happens and countless Americans will perish in the process. Any member of Congress who does not move to impeach Biden over this is abrogating their constitutional duty.” (Biden Administration Negotiates Deal To Give WHO Full Authority Over U.S. Pandemic Policies.)
No one should be holding their breath over an impeachment of President in Name Only Joseph Robinette Biden, Jr., which is simply not going to happen, especially when one considers that the Republican likes of Addison Mitchell McConnell, Willard Mitt Romney, Thomas Roland Tillis, John Cornyn, and Susan Collins love to enable the Deep Security State at home and the agenda of globalists worldwide. It will not be too terribly far into the future before some globalist statist will declare a “climate emergency” that will make the repressive measures associated with the CCP/Wuhan/SARS-CoV-2/Covid-19/Coronavirus seem like so much child’s play.
Moreover, the treaty that is being negotiated to give the World Health Organization total control over the world's so-called "healthcare" system but also over the ability of private individuals and farmers to raise their own chickens and livestock in those nations that become signatories to the treaty:
This should have your attention full stop because the WHO is gearing up to give itself the authority to declare pandemics and to control this country’s pandemic response. As I reported in a post published earlier today, the WHO has published a draft of the pandemic accord the Biden administration fully intends to enter into.to declare pandemics and to control this country’s pandemic response. As I reported in a post published earlier today, the WHO has published a draft of the pandemic accord the Biden administration fully intends to enter into.
Tedros: "Next week, countries will begin negotiations on a 'Zero Draft' of the new Pandemic Accord." Once agreed, this "Accord" will subvert all Nations sovereignty and hand it over to the globalists in the WHO. . pic.twitter.com/IGbx7b8tzq — Dr. Anastasia Maria Loupis (@DrLoupis) February 22, 2023
What I didn’t dive into is the concerning language that gives the WHO not only the authority to impose mandatory vaccines and lockdowns but allows it to use “viruses” in animals and the threat of a “pandemic” to take over U.S. livestock and our food supply.
The WHO is already letting us know they’re going to start with poultry—and you’re either going to allow your flocks to be controlled, surveilled, and vaccinated, or they’ll be killed so the viruses they don’t have won’t spread to people (or harm the environment). They are already laying the groundwork for this, and the authority they’ll derive this power from is the pandemic accord.
If you read through the 32-page draft of the accord, you’ll see how this document gives the WHO the authority to take control over U.S. agriculture and our food supply:
By signing onto the accord, a country acknowledges that “most emerging infectious diseases originate in animals, including wildlife and domesticated animals, then spill over to people.” (See p. 6)
From the outset, they’re laying the foundation that “most infectious diseases” begin in animals; thus, their ability to regulate animals is within their purview.
Parties must reaffirm the importance of a “One Health approach” to detect and prevent health threats at the animal and human interface, “in particular zoonotic spill-over and mutations, and to sustainably balance and optimize the health of people, animals, and ecosystems.” (See p. 6)
In other words, a member state that signs on to the accord has to agree to drink the Kool-Ade. They don’t want member states dissenting, so everyone needs to “reaffirm” their loyalty to an initiative called the “One Health Approach,” whose scope includes the health of people, animals, AND ecosystems.
Parties must acknowledge “the creation of the Quadripartite” to “better address any One Health-related issue.”
Here, you see who will have the “authority” over food and agriculture. It’s not the United States Department of Agriculture, Congress, your states, landowners, or farmers. It’s not even your elected officials or U.S. citizens.
The draft states explicitly that the “Quadripartite” consists of the WHO—whose top three donors include the U.S., Bill and Melinda Gates Foundation, and the People’s Republic of China—the Food and Agriculture Organization of the United Nations, the World Organisation for Animal Health, and the United Nations Environment Programme.
By signing this accord, a country must commit to integrating a “One Health surveillance system [. . .] to identify and assess the risks and emergence of pathogens and variants with pandemic potential, in order to minimize spill-over events, mutations and the risks associated with zoonotic neglected tropical and vector-borne diseases, with a view to preventing small-scale outbreaks in wildlife or domesticated animals from becoming a pandemic (page 24).”
Furthermore, each party shall “foster actions at national and community levels that encompass whole-of-government and whole-of-society approaches to control zoonotic outbreaks (in wildlife and domesticated animals), including engagement of communities in surveillance that identifies zoonotic outbreaks and antimicrobial resistance at source.”
The sections that follow discuss how parties must enhance surveillance to “identify and report pathogens” and strengthen “infection prevention and control in health care settings and sanitation and biosecurity in livestock farms […].”
In other words, if you have your own animals, the WHO is going to know about it and have control over them because . . . viruses.
According to the WHO’s website, OneHealth is an “integrated, unifying approach to balance and optimize the health of people, animals, and the environment. It is particularly important to prevent, predict, detect, and respond to global health threats such as the COVID-19 pandemic.”
OneHealth “involves the public health, veterinary, public health, and environmental sectors” and is “particularly relevant for food and water safety, nutrition, the control of zoonoses […], pollution management, and combatting antimicrobial resistance […].”
A One Health High-Level Expert Panel was formed in May 2021 to advise the WHO and other agencies on “One Health” issues. If these “advisors” are anything like the CDC or FDA’s vaccine advisors, we can expect that they have questionable ties to the WHO, Bill Gates, and pharmaceutical companies—and are merely there to enforce the WHO’s agenda.
The WHO’s website further states:
“Critical areas this panel addresses include food production and distribution, urbanization and infrastructure development, international travel and trade, activities that lead to biodiversity loss and climate change, and those that put increased pressure on the natural resource base — all of which can lead to the emergence of zoonotic diseases.”
Do you see what the WHO is doing here? How clever to slide language into a pandemic accord that requires parties to ascribe to this One Health agenda—that is not explained at all in this draft.
The WHO isn’t just putting itself in charge of pandemics; they’re using the reality that some viruses originate in animals to take control of livestock and the food supply—and giving themselves the broad authority to do so in the name of viruses, “biosecurity” and even climate change.
Given Bill Gates is the second largest donor of the WHO and wants “rich nations” to eat “100% synthetic beef” and genetically modified plant-based toxin burgers, this should give you pause. This pandemic accord is the vehicle by which all of the ridiculous initiatives peddled by the elite at the World Economic Forum will be carried out.
This accord will, if entered into by the U.S., usurp our nation’s sovereignty, violate our privacy, restrict our independence, and infringe upon our right to grow our own food and raise our own animals. Everything will be done in the name of a “pandemic,” and we will be powerless to stop it. (WHO’s Pandemic Accord Will Give It Control Over U.S. Livestock and Food Supply – Site Title.)
Although we might be powerless in earthly terms to stop this madness, we are never "powerless" supernaturally if we rely upon the intercessory power of Our Lady, Saint Joseph, our Guardian Angels, patron saints, and the entire cloud of witnesses in the Church Triumphant in Heaven as well as in the Church Suffering in Purgatory to help us to prosper spiritually no matter what we are called to suffer in this passing, mortal vale of tears as nothing we suffer here is the equal of what one of our least Venial Sins caused Our Blessed Lord and Saviour Jesus Christ to suffer during His Passion and Death on the wood of the Holy Cross and that caused His Most Blessed Mother to suffer in perfect communion with Him as our Co-Remeptrix, Advocate, and Mediatrix of All Graces.
II. Wuhan "Vaccines": Recpie for Death and Injuries
The second part of this ongoing genocide, of course, involves the development of “emergency use” “vaccines,” each of which was developed from stem cell lines derived originally from butchered human embryos, that have not only not prevented people from getting the virus but whose spike protein in the mRNA messenger jabs have spread the virus to the unvaccinated and resulted in long term medical conditions such as myocarditis for the jabbed. Many others of the jabbed are dealing with “long Covid,” something that Dr. Peter A. McCullough wrote as follows on Thursday, February 16, 2023:
The global COVID-19 pandemic was characterized by global spread from acutely ill to susceptible population in well-known “hotspots” including Wuhan, Milan, New York, etc. Australia’s turn at surges in cases occurred late as the majority of the population had received one or more of the failed COVID-19 vaccines. Thus, post-COVID syndromes in Australians invariably include the long-term consequences of he vaccines superimposed by one or more occurrences of the infection. In fact, prior vaccination is likely to make post COVID syndromes far worse in a process termed Vaccine Associated Enhanced Disease (VAED). The Australian Senate has commissioned an inquiry into long COVID-19, and now a written submission for the terms of reference published by Dr. Melissa McCann will cause the process to stratify and consider post COVID-19 syndromes according to the additional exposure of COVID-19 vaccination.
This is an important development as clinicians were concerned that the inquiry was a means to “cover up” vaccine injuries in a broad bucket of long COVID-19 syndromes with no mention of the vaccines. McCann points out in her submission that after the infection that the S1 segment of the SARS-CoV-2 Spike protein is found within monocytes. Conversely if a vaccine has been received, both the S1 and the pathogenic S2 segment will be within the body.
It has been my experience that every vaccine injection and each occurrence of COVID-19 respiratory illness count in a cumulative exposure of SARS-CoV-2 Spike protein which drives the risk for cardiovascular, neurological, immune system, and hematological complications. Most of these emerge within 30 days of the most recent Spike protein exposure. Thus post-COVID syndromes are both a product of vaccination and the respiratory infection. Only careful epidemiologic and laboratory analysis will determine the relative contributions of these determinants to the occurrence, severity, and consequence of each long COVID syndrome. (Long COVID-19 to Include Vaccine Associated Enhanced Disease.)
Additionally, as is well known, the vaccines have caused a global epidemic of sudden deaths, about which very few people seem to have the least bit of curiosity to seek an explanation. “Died suddenly” has now become an accepted part of the news and obituaries, and only a handful of people see any connection between the effects of the poisoned injections and the fact that people of all ages, including teenagers and young adults, are dying “suddenly”:
A new and increasingly popular Twitter hashtag is “#diedsuddenly” in response to a surge of sudden unexplained deaths among mostly young and healthy individuals, including athletes, occurring over the past 2 years. Here are but a few recent news stories.
In Australia, “Fit and healthy 21 year old son dies suddenly in his sleep.” From the University of Arizona, “A recent member of Arizona’s men’s swim team has unexpectedly passed away.” In Detroit, a high school basketball player suffered a cardiac arrest during a basketball game. While they restarted his heart, he hasn’t woken up.
Or this athlete in his early 20’s, “A former Florida Gators offensive lineman died suddenly on Thursday night according to multiple media reports.” From the US Army, “A soldier stationed at Fort Stewart died Tuesday while traveling to California for a training exercise.” Is this some type of black magic? Not likely, “America’s Got Talent magician suddenly dies at just 52.”
Let’s not forget Buffalo Bills player Damar Hamlin going into cardiac arrest after an unremarkable tackle during a January NFL game. These are anecdotes, and while compelling are not the same as collected data.
Several brave researchers recorded these “sudden” and “unexplained” deaths, as they are described in the media. Here is one report, “An investigation of official statistics has found that the number of athletes who have died since the beginning of 2021 has risen exponentially compared to the yearly number of deaths of athletes officially recorded between 1966 and 2004.”
This trend was quite worrisome, “So much so that the monthly average number of deaths between January 2021 and April 2022 is 1,700% higher than the monthly average between 1966 and 2004.”
Where are the 3-letter health agencies? Why haven’t the FDA, NIH, or CDC offered their own data to refute this alleged increase in sudden deaths? If this is all “misinformation” as big tech and the corporate media describes it, the health agencies should easily be able to disprove it, rather than calling on social media giants to censor or ban anything contrary to their “safe and effective” mantra.
Big Medicine and the media attempt to play this all off as normal but average Americans are noticing and are understandably concerned. Since when is it “normal” for high school and college athletes to have heart attacks and blood clots, often fatal? Why are these daily news stories now compared to years ago when one might hear of only a few cases per year, typically attributed to a previously undiagnosed congenital heart defect? Why are these deaths frequently “unexplained” leaving “doctors mystified”?
America has the best medical care in the world and few medical maladies remain “unexplained” in 2023, other than the recent surge in sudden deaths among the young and healthy.
Are people noticing? Rasmussen Reports asked Americans what they think about all of this. In a national telephone and online survey of 1000 adult Americans published a month ago, four questions were asked.
- Have you received a COVID-19 vaccination?
- How likely is it that side effects of COVID-19 vaccines have caused a significant number of unexplained deaths?
- Do you personally know anyone whose death you think may have been caused by side effects of COVID-19 vaccines?
- Which is closer to your belief, that there are legitimate reasons to be concerned about the safety of COVID-19 vaccines, or that people who worry about vaccine safety are spreading conspiracy theories?

How did they answer? 71% of those surveyed were vaccinated, comparable to the national average. Virtually half of respondents don’t believe the “disinformation” mantra propagated by “fact checkers”, mainstream media, and the government. “49% of American adults believe it is likely that side effects of COVID-19 vaccines have caused a significant number of unexplained deaths, including 28% who think it’s very likely.”
Furthermore, “28% of adults say they personally know someone whose death they think may have been caused by side effects of COVID-19 vaccines.” And “48% of Americans believe there are legitimate reasons to be concerned about the safety of COVID-19 vaccines.”
The 2022 film “Died Suddenly” reinforces the above concerns, despite critics describing the movie as “baseless”, “propaganda”, or “pseudoscience”. Maybe it is, maybe not. If this is all nonsense, it should be as easy to disprove as it would be to dispel the notion that the sun orbits the earth, rather than vice versa.
Why doesn’t the CDC do a simple analysis, as Steve Kirsch has suggested, linking death and vaccination records? Kirsch has even offered a 10X return on a bet anyone wants to make with him disproving his analysis or conclusions. Any takers?
Since COVID-19 began 3 years ago, trust in medical authorities has declined. According to Pew Research, “29% of U.S. adults say they have a great deal of confidence in medical scientists to act in the best interests of the public, down from 40% who said this in November 2020.”
Much of what we have been told over the past few years has turned out to be false. A recent Cleveland Clinic study found that more vaccine doses lead to a greater likelihood of getting COVID-19. Or a Cochrane analysis concluding that masks in the community made “little to no difference” in COVID-19 infections or deaths. Weren’t we told otherwise by authoritative doctors in white coats? Challenges to the approved party line were met with threats to one’s medical license, job, or reputation.
Someday there will be another public health emergency and it would behoove health authorities to set the record straight, either proving their assertions, or admitting they were wrong and thoughtfully analyzing why. Otherwise, they will have little future credibility, much like the boy who cried wolf. (So many people recently ‘died suddenly’ – What’s going on?.)
Officials in Australia have confirmed that the nation’s first openly gay Olympic bobsledder, Simon Dunn, died suddenly at age 35.
Dunn’s body was reportedly found at his home in Sydney on Saturday. Police do not feel the death is suspicious and are going on the assumption that there is a medical reason for the passing, according to Yahoo Sports.
Ruby Rose Management confirmed the news with a statement saying, “About 10 am on Saturday, January 21, 2023, police were called to a unit on Crown Street, Surry Hills, after reports the body of a man had been found inside. The body is believed to be that of the 35-year-old occupant. Officers from Surry Hills Police Area Command have commenced inquiries into the circumstances surrounding his death, which is not being treated as suspicious.”
Dunn rose to fame in 2014 when he became the first openly gay member of the country’s Olympic bobsledding team. After retiring from the team in 2016, Dunn played for an all-gay rugby team, engaged in media appearances, and explored acting.
In 2021, Dunn attempted to make a bobsledding comeback by working to join the Australian team for the 2022 Winter Olympics. But his dream was dashed when he ruptured a bicep muscle during training. (Simon Dunn, Famed Australian Olympian and Rugby Player, Dies Suddenly at 35.)
Dr. Joseph Mercola reported on this phenomenon as follows in his posting of January 16, 2023:
- Over the past two years (2021 and 2022), more than 1,650 professional and amateur athletes have collapsed due to cardiac events and 1,148 of them proved fatal
- Damar Hamlin, a 24-year-old Buffalo Bills football player went into cardiac arrest on live television after being tackled during a January 2, 2023, game against the Cincinnati Bengals. Team trainers and emergency medical staff performed CPR for more than nine minutes, which saved his life
- Whether the COVID jab played a role in what happened to Hamlin is impossible to know for sure, but Dr. Peter McCullough suspects it may have played a role — provided he actually got the shot
- A condition called commotio cordis is known to occur in baseball when a player is hit hard on the breastbone, thereby causing cardiac arrest. There are approximately 20 to 30 such cases each year, but never in pro football. In McCullough’s view, commotio cordis can likely be ruled out. The more likely cause for Hamlin’s cardiac arrest, he believes, is hypertrophic cardiomyopathy (HCM), or abnormal thickening of the heart muscle, which is the primary cause for athletes suffering cardiac arrest
- During exercise, adrenaline is pumping, and when the heart is damaged this adrenaline rush is what triggers the cardiac arrest. This helps explain not only the death of athletes on the field, or people dying while jogging, but also why so many are dying in their sleep, because adrenaline is released between 3 a.m. and 6 a.m., as your body readies to wake up.
With every passing day, the list of people suffering tragic consequences from the COVID mRNA shots grows longer. As of December 23, 2022, the U.S. Vaccine Adverse Events Reporting System (VAERS) had received 33,334 reports of post-jab deaths, 26,045 cases of myocarditis and 15,970 heart attacks.1
Many of these people and their stories have remained hidden from public view as social media have universally censored these stories. As a result, people who only read mainstream media are largely unaware of the damage being done. However, there is a population of people whose injuries and deaths have been far more public.
Over the past two years (2021 through 2022), more than 1,6502,3,4,5,6,7 professional and amateur athletes have collapsed due to cardiac events and 1,1488 of them proved fatal. In his book “Cause Unknown: The Epidemic of Sudden Deaths in 2021 and 2022,”9 Edward Dowd writes extensively about the anomalous number of deaths now occurring among athletes, which, despite “fact checkers” best efforts to dismiss it as “normal,”10,11 is anything but.
What Happened to Damar Hamlin?
More than likely, you’ve heard that Damar Hamlin, a 24-year-old Buffalo Bills football player went into cardiac arrest on live television after being tackled during a January 2, 2023, game against the Cincinnati Bengals.12,13 Team trainers and emergency medical staff performed CPR for more than nine minutes, which saved his life. After initially being placed in a medically-induced coma, Hamlin was reportedly on the mend within a week.14
Whether the COVID jab played a role in what happened to Hamlin is impossible to know for sure. Looking at the replays, it’s clear he took a very severe hit right to the chest right before his collapse, and this certainly could have caused the heart attack. At bare minimum, it’s not unheard of. Former Pittsburgh Steelers linebacker had a similar incident in 2017, as did hockey legend Chris Pronger in 1998.15
On the other hand, it’s also not inconceivable that the COVID jab — if Hamlin was in fact “vaxxed” — could have affected his heart, thereby playing a contributing role. We now know the COVID shot is associated with a significantly elevated risk of myocarditis, which in turn raises the risk of sudden cardiac death in contact sports.16
While the NFL enforced strict COVID jab rules for employees who have contact with players, the players and coaches were not subject to mandates.17,18 That said, 95% of players did get the shot, according to the NFL league.19
Cardiologist Offers His View
In a January 4, 2023, Children’s Health Defense interview, Dr. Peter McCullough, a cardiologist and internist, reviewed what could have happened in Hamlin’s case. As noted by McCullough, a condition called commotio cordis (Latin for “agitation of the heart”) is known to occur in baseball when a player is hit hard on the breastbone, thereby causing cardiac arrest. There are approximately 20 to 30 such cases each year.
However, no such case has ever occurred in 100 years of pro football. Football players have padding that protects the breastbone, so in McCullough’s view, commotio cordis can likely be ruled out. The more likely cause for Hamlin’s cardiac arrest, he believes, is hypertrophic cardiomyopathy (HCM), or abnormal thickening of the heart muscle, which is the primary cause for athletes suffering cardiac arrest.
The reason why HCM is the No. 1 cause of cardiac arrest in professional athletes is because it causes few if any symptoms and often goes undiagnosed. Professional athletes undergo extensive medical evaluation and cardiovascular screening20 before being given the green-light to play, and they also constitute the healthiest segment of society in general,21 so most heart problems are ruled out before they ever enter the field.
“The elephant in the room,” however, according to McCullough, is the COVID jab. Before these shots were rolled out, the average number of cardiac arrests in all European soccer and football leagues combined was 29 per year. Since the advent of the COVID shots, 1,598 European pro athletes have suffered cardiac arrest, giving us a comparative annual tally of nearly 800. Of those 1,598 cardiac arrests, 1,101 were fatal.
McCullough detailed these and other stats in a December 17, 2022, letter to the editor of the Journal of Scandinavian Immunology. The paper was co-authored by Panagis Polykretis, Ph.D., a researcher at the Institute of Applied Physics, which is part of the Italian National Research Council.22 McCullough and Polykretis have been, and still are, calling for a proper investigation of these deaths.
McCullough Suspects COVID Jab-Induced Myocarditis
McCullough and Polykretis suspect COVID jab-induced myocarditis is the explanation for this otherwise inconceivable increase in cardiac arrests among athletes, and McCullough believes it also tops the list of potential reasons for Hamlin’s cardiac arrest, considering 95% of NFL players had received the jab as of March 2022.23
McCullough cites research showing about 2.5% of COVID jab recipients sustain heart damage, 90% of them being men. And, in about half of all jab-related myocarditis cases, there are no symptoms to alert you there might be a problem. As explained by McCullough, myocarditis causes scarring on the heart, and it is this scarring that causes an abnormal electrical rhythm (ventricular tachycardia) and sudden adult death syndrome.
There are now more than 200 scientific papers on jab-related myocarditis. A January 2023 study24 in the European Journal of Pediatrics found high levels of circulating spike protein in 16 male high school students hospitalized with myocarditis induced by the shots, which again suggests the spike protein your body produces is a key pathogenic factor.
McCullough explains in greater detail how the shot may have triggered Hamlin’s cardiac arrest: During play, adrenaline is pumping, and when the heart is damaged this adrenaline rush is what triggers the cardiac arrest.
This helps explain not only the death of athletes on the field, or people dying while jogging, but also why so many are dying in their sleep, because adrenaline is released between 3 a.m. and 6 a.m., as your body readies to wake up.
1,696% Increase in Sudden Death Among Athletes
Whatever caused Hamlin’s cardiac arrest — and hopefully a careful medical investigation after his recovery will clarify what happened — there’s no doubt that athletes in general are dying in far greater numbers now than ever before.
The number of athletes who ‘died suddenly’ between January 2021 and April 2022 was 1,696% above the historical monthly norm between 1966 and 2004 — 42 per month compared to just 2.35 per month.
In related news, a November 2022 report25 by The Exposé showed the number of athletes who “died suddenly” between January 2021 and April 2022 was 1,696% above the historical monthly norm26 between 1966 and 2004 — 42 per month compared to just 2.35 per month.
Risk of Cardiovascular Damage Soars After Second Shot
A nearly 1,700% increase in sudden cardiac-related death among athletes is inexplicable unless you take the experimental COVID jabs into account. Research28 published in November 2021 found inflammatory markers — signs of cardiovascular damage — rose dramatically after the second COVID shot, and the risk of heart attacks and other heart-related problems more than doubled in the months following these injections.
Pre-jab, patients had an 11% five-year risk of heart attack. Post-jab, that risk rose to 25%, a 227% increase in risk. As reported by The Exposé, other statistics also reveal heart damage has become ubiquitous among those who got one or more mRNA jabs:29
“Acute cardiac failure rates are now 475 times the normal baseline rate in VAERS. Tachycardia rates are 7,973 times the baseline rate. Acute myocardial infarction is 412 times the baseline rate.
The rates of internal hemorrhage, peripheral artery thrombosis, and coronary artery occlusion are all over 300 times the baseline rate … It doesn’t take a genius to work out that COVID-19 vaccination is the reason the monthly average number of athlete deaths was 1,700% higher than the expected rate by April 2022.”
Sudden Death: The No. 1 Cause of Death for Under 65s in 2021
In late December 2022, Steve Kirsch also published data showing the shots are a public health disaster.30 According to the results of a survey Kirsch conducted, “sudden death” was the No. 1 cause of death in 2021 and 2022 among Americans under 65 who had received the COVID shot.
The second and third causes of death in this group were cardiac-related death and cancer respectively. Importantly, the incidence of turbo-charged cancer among the jabbed was also significant, and myocarditis killed more than COVID-19.
Among the unjabbed, the primary cause of death for people 65 and younger in 2021 and 2022 was hospital treatment for COVID. Incidences of sudden death, pulmonary embolism and turbo-charged cancers were all low, and there were no unknown causes of death, nor any myocarditis deaths. Kirsch summarized the three most stunning differences between the jabbed and unjabbed as follows:31
- “Sudden death rates are off the charts for the vaccinated cf. unvaccinated for those <65 … It’s the #1 cause of death for this age group …
- Myocarditis as a cause of death is registering now for both age ranges but only for the vaccinated …
- Cardiac issues as a cause of death in vaccinated young people (<65) are significantly elevated vs. their unvaxxed peers.” (Fact Checkers Can't Hide It, Sudden Deaths Soar 1,696% .)
Yet another study that focused on autopsy results provides further documentation of how the poisoned jabs have killed people by means of myocarditis:
A serious side effect linked to COVID-19 vaccines can lead to death, according to a new study.
Post-vaccination myocarditis, a form of heart inflammation, was identified in a subset of people who died “unexpectedly” at home within 20 days of receiving a COVID-19 vaccine.
Researchers analyzed autopsies that had been performed on the people and conducted additional research, including studying tissue samples.
Researchers started with a group of 35, but excluded 10 from further analysis because other causes of death were identified. Of the remaining 25, researchers identified evidence of myocarditis in five.
All of the five people received a Moderna or Pfizer vaccine within seven days of their death, with a mean of 2.5 days.
The median age was 58 years. None of the people had COVID-19 infection prior to being vaccinated and nasal swabs returned negative.
Autopsy findings combined with the lack of evidence of other causes of death and how the vaccination happened shortly before the deaths enabled researchers to say that for three of the cases, vaccination was the “likely cause” of the myocarditis and that the cardiac condition “was the cause of sudden death.”
In one of the other cases, myocarditis was believed to be the cause of death but researchers detected a herpes virus, an alternative explanation for the incidence of heart inflammation.
The remaining case did not include an alternative explanation for the myocarditis but the researchers said the impact of the inflammation was “discrete and mainly observed in the pericardial fat.”
They classified the two cases as possibly caused by vaccination.
“In general, a causal link between myocarditis and anti-SARS-CoV-2 vaccination is supported by several considerations,” the researchers said, including the “close temporal relation to vaccination”; the “absence of any other significant pre-existing heart disease”; and the negative testing for any “myocarditis-causing infectious agents.”
Limitations included the small cohort size.
The study was published by Clinical Research in Cardiology on Nov. 27. The researchers all work for Heidelberg University Hospital. They were funded by German authorities.
Moderna and Pfizer did not respond to requests for comment.
The meticulous ruling out of possible causes apart from vaccination signals that the cases are “the tip of the iceberg,” Dr. Andrew Bostom, a heart expert based in Rhode Island, told The Epoch Times.
“If there’s a seemingly healthy person that dies suddenly in their sleep, essentially, these are typically the cases that are autopsied, and clearly the most common finding is some form of atherosclerotic coronary heart disease. But they basically ruled that out in these cases. And then they came up with the most plausible proximate cause being vaccination,” he said.
“And so it suggests that the phenomenon could actually be broader than it’s been suspected to be.”
Myocarditis
Myocarditis is a serious heart condition that can manifest as chest pain and typically leads the sufferer to seek hospital care.
Doctors usually advise against all or most physical activity for a period of time.
Causes include bacteria, viruses and fever.
Acute myocarditis resolves in about half of cases in the first two to four weeks, researchers have found, but another quarter feature longer-term problems and many of the rest lead to death or heart transplantation.
The incidence of myocarditis among COVID-19 vaccine recipients was higher than expected, researchers in the U.S., Israel and other countries have found.
The highest rates have been detected in young people, particularly young males.
Estimates of the typical myocarditis incidence rates are 0.2 to 2.2 per million persons within seven days.
Reports to the Vaccine Adverse Event Reporting System show higher rates for males aged 5 to 49 and females aged 12 to 29.
The highest rate was 75.9 per million-second doses administered. Reports to the system don’t prove causality but the system suffers from severe underreporting, according to studies, indicating the rates are even higher.
The Centers for Disease Control and Prevention (CDC) continues to recommend vaccination for virtually all people aged 6 months and older, asserting that the benefits of the vaccines outweigh the risks.
Some experts disagree, saying side effects like myocarditis tilt the calculus to the risks being higher in some age groups.
Government officials have repeatedly said that most of the myocarditis cases resolve within weeks, but CDC researchers found in September that many youths who experienced post-vaccination myocarditis still had abnormal MRI results months later.
The incidence has been much lower among older people, according to U.S. authorities, which have refused to make public the autopsy results of people who die after vaccination and various studies.
The new study “suggests we’ve been missing some severe myo[carditis] cases in our studies,” Dr. Tracy Høeg, an epidemiologist who advises the Florida Department of Health, said on Twitter.
Causality
Several vaccines have been linked to myocarditis and a related condition, pericarditis. They are made by Moderna and Pfizer and are the two most widely administered in the U.S. and Germany.
Both vaccines utilize messenger RNA (mRNA) technology.
Causality means that a vaccine causes a condition.
Top CDC researchers have said the current evidence shows a causal link between the mRNA shots and heart inflammation. Other researchers have also reached that conclusion.
The U.S. Food and Drug Administration warns potential vaccine recipients that “postmarketing data demonstrate increased risks of myocarditis and pericarditis, particularly within 7 days following the second dose.”
Bostom said the evidence he’s reviewed shows a causal link.
“It’s as certain as most associations that we say are confirmed in medicine,” he said.
Some studies have identified COVID-19 as another cause of myocarditis and pericarditis, but others have indicated it might not be associated.
Other Autopsy Findings
Before the German study, other researchers around the world had reported findings from autopsies of people who died suddenly after vaccination.
In 2021, U.S. researchers reported two adults developed myocarditis within two weeks of COVID-19 vaccination, and they were unable to find causes other than vaccination.
In 2021, South Korea researchers reported that after examining the death of a 22-year-old man who died five days after receiving the Pfizer vaccine, they determined the primary cause was “myocarditis, causally-associated” with the vaccine.
In January, New Zealand researchers reported that the Pfizer vaccine was probably responsible for sudden myocarditis that led to the death of a 57-year-old woman, writing that “other causes have been discounted with reasonable certainty.”
In February, researchers in several U.S. states reported that two teenage boys who died shortly after receiving Pfizer’s vaccine experienced heart inflammation and that the inflammation was the primary cause of death.
In May, CDC researchers reported that a young boy died after experiencing post-vaccination heart inflammation, with myocarditis being pegged as the cause of death.
In September, a German researcher reported that a 55-year-old who died four months after receiving the Pfizer vaccine died of myocarditis and said “these findings indicate that myocarditis, as well as thrombo-embolic events following injection of spike-inducing gene-based vaccines, are causally associated with a[n] injurious immunological response to the encoded agent.”
And just recently, Japanese researchers reported on results from a 27-year-old man who died 28 days after admission following vaccination. (Autopsies Show COVID Vaccine Caused Fatal Cardiac Condition in Some People.)
As noted earlier, the epidemic of excess and sudden deaths is global, something has been document in Europe just for the month of December, 2022, has been noted by, of all things, the European Union’s statistic arm, Eurostat:
Eurostat has published the excess mortality for the month of December 2022, where the European average is over 19%, with Romania and Bulgaria being the only states with a decrease in this parameter.
The reporting was done on an average of mortality in the period 2016-2019, pre-pandemic years. The countries with the most catastrophic excess death rates are Iceland and Germany, up 43.1% and up 37.3%, respectively.
The data published by Eurostat shook the entire scientific world. At the end of the pandemic, when Covid deaths are almost non-existent, the most vaccinated countries recorded horror percentages of excess mortality in December 2022, compared to the period of normality 2016-2019.
The highest percentages of excess mortality were recorded in Iceland, with an increase of 43.1%, and in Germany, with an increase of 37.3%. Compared to the December 2022 European average of 19%, which is huge anyway, Austria had excess mortality of 27.4%, Ireland 25.4%, France 24.5%, Slovenia 25,9%, Czech Republic, 23.2%, Switzerland, 22.9%, Netherlands, 22.7% Estonia, 22.6%, Denmark, 22.4%, Norway, 21%, Finland, 21.1%, Latvia, 20.6% and Belgium, 19.1%.
Germany has 78% of the population vaccinated with 3 and 4 doses, and Iceland has 80% of the population vaccinated with 2 doses and 69% of the population vaccinated with 3 and 4 doses. At the opposite pole of excess mortality from December 2022 were Romania and Bulgaria, which had minus 5.5% and minus 6%, respectively, these being the only two EU/EEA states that vaccinated the least. Officially, Bulgaria has 30% of the population vaccinated against Covid, and Romania has 42%.
Given the negative percentages of excess mortality close between the two countries, taking into account fictitious vaccinations from Bulgaria, the real percentage of vaccinated people in Romania is somewhere at most 25%.
After Eurostat published the shocking data, doctors in Germany called for an investigation into the causes of the excess deaths, stressing that they were not caused by Covid.
They hid the disaster
Things are even worse than that. Germany had, in the last week of December last year, excess mortality of over 46%. Eurostat data clearly showed a correlation between the percentage of anti-Covid vaccination and that of excess mortality.
The higher the degree of vaccination, the higher the excess mortality.
It is curious that Italy and Sweden did not report to Eurostat and have not reported since August-September 2022. Portugal reported in December 2022 a plus 14.8% excess mortality, but they had over 40% in the summer because they also vaccinated the population earlier than the other countries.
The UK tried to skew the actual percentage of excess mortality by taking the reporting period from 2016-2019 and 2021. So they put the year with the highest mortality into the calculation basis.
The vaccine increased mortality
Official data shows that in 2021, 4.5 billion people worldwide received one dose of the Covid vaccine, 3.8 billion received two doses and 537 million received three doses. However, compared to 2020 when there was no vaccine, 2021 saw the most Covid deaths reported. Thus, if in 2020 there were 1.9 million Covid deaths, in 2022, the number was 3.4 million. It is perhaps the most eloquent evidence that the vaccine did not work in any way and that it did not protect anyone, but, on the contrary, managed to increase mortality enormously.
In 2022, only one billion people have received one dose of the Covid vaccine, less than one billion have had two doses, and 2.3 billion have received the third and fourth doses. At the level of 2022, only 1.1 million Covid deaths were reported, but with high percentages of excess mortality rate. (Excess Deaths Explode in Vaccinated Countries. Romania and Bulgaria Are in the Red.)
The empirical statistics speak for themselves, and they are buttressed by the following anecdotal accounts drawn from obituaries in just one small region (the names of the individual people and their places of death have been omitted and replaced with made up names).
- [Arthur Stanley Jefferson] passed away unexpectedly at his home. He was 49.
- [Arthur Justin], 75, passed away unexpectedly at home.
- [Tracy Oliver] died suddenly at the age of 44.
- [Barbara Richards], age 60, passed away at her.
- [Frances Belding], 74, of Haydenville, died after developing Creutzfeldt-Jakob disease two months earlier. She died peacefully at home surrounded by her loved ones.
- [Rocco DeBellis], 59, unexpectedly passed away early Sunday morning.
- [Carl Riese], 56, passed away at his home.
- [Suzanne Dwyer], 61, died unexpectedly on Saturday.
- [Buddy Berkelmann], 70, passed away unexpectedly at his home on Wednesday.
- [George Olchefsky] was called home, unexpectedly.
- [Rebecca Yarmy], 62, died unexpectedly, while sitting at the desk in her office.
- [Betsy Cullen], 40, passed away unexpectedly on Friday.
- [Sylvia Schnauser] passed away peacefully (but unexpectedly) on Sunday.
- [Brian Flynn], 65, passed away unexpectedly home.
- [John Trask] died suddenly on Monday while he was working on his computer.
It would be intellectually dishonest to claim that each of these days was caused in one way or another by the vaccines as some of those who “died suddenly” or “died unexpectedly” may not have gotten jabbed. However, as one who is seventy-one years, three months of age, I, for one, have never seen such a spate of “sudden deaths” confined to just one small part of a geographic region. Moreover, this phenomenon is not something provincial. It is global, and it is almost as though the major obituary services have templates for funeral home directors to use when writing obituaries and/or when instructing relatives how to do so. The lack of intellectual curiosity about these deaths just boggles the mind.
Additionally, the vaccines have not only killed many untold thousands of people, but they have also injured untold thousands of people, including a fitness expert in the United Kingdom who has not been the same since he got vaccinated for the coronavirus:
Adam Rowland had a promising career, working with professional athletes on the PGA Tour and Premiership Rugby, splitting his time between the U.S. and the U.K.
He also was the fittest he’d ever been, Rowland told The Defender — until early 2021, when he received the two-dose primary series of the AstraZeneca COVID-19 vaccine.
Today, Rowland, 48, cannot work, cannot lie down, and experiences several conditions affecting everything from his heart health to his vision, including pericarditis, pulmonary embolisms, severe thrombotic vasculitis and vascular neuropathy.
He is now separated from his wife, misses most family events and was repeatedly told by doctors that his severe injuries were “all in his head” — bringing him to the brink of suicide.
He said his discovery of online support groups for the vaccine-injured afforded him a new lease on life.
Rowland, who provided extensive documentation supporting his claims, shared his story with The Defender in an exclusive interview.
‘I was the fittest I’d ever been in my life’
Rowland had worked as a medical sports physiotherapist and stroke consultant for professional golfers for the previous 16-17 years.
“I was absolutely at the top of my career in professional sport,” he said, having worked on the PGA Tour with Jason Day and other high-profile golfers.
“I was working in America when COVID kicked off,” said Rowland, “and living quite a luxury lifestyle. And then, I decided to come back to the U.K. because obviously, I didn’t know when I’d be able to get back to the U.K. if I didn’t go then.”
The U.S. government gave Rowland special permission to return to the country and resume his employment. However, “Once the vaccination program kicked in, you had to be double vaccinated.”
It was during this time — before he got the vaccine — that Rowland said he was “even fitter than when I was 18,” because “any workout program I gave an athlete, I would try it myself” to determine firsthand how physically strenuous it was.
He said:
“So, because of that, I exercised six or seven days a week … I was just so fit, I could row on the rowing machine 18 minutes, something around five kilometers. I could ride a bike 20K in under 30 minutes. At one stage I was running 5K in 21 minutes.”
Multiple injuries and conditions brushed off as ‘anxiety’
Rowland received two doses of the AstraZeneca COVID-19 vaccine in February and May 2021. That’s when everything changed.
“Very quickly after being vaccinated, I started to get quite ill,” said Rowland. “I never got back to the U.S.” He continued working for six months after his first dose, but had to take a lot of time off from work because he was in the hospital.
“I’ve never worked since,” he said. “I’ve lost my job and I’m disabled as we speak.”
Rowland’s symptoms began with a “fever like I’d never had before in my life,” he said. “I was in bed for four days.” The fever eventually subsided, he said, “but I felt very virally ill for a number of weeks. I started to notice horrendous pains down my left arm and my left leg. And my wife noticed I started to have fits in bed … they were basically non-epileptic fits.”
The symptoms appeared within a week of his first dose.
Rowland couldn’t get a face-to-face appointment with his doctor because of the pandemic, so he had to settle for a phone appointment. The doctor diagnosed him with “anxiety” and “said it was a panic attack” — not unlike what happened to other vaccine-injury victims, whose conditions also were chalked up to “anxiety.”
Rowland’s condition continued to worsen. “I couldn’t sleep for five days because [the fits] were happening 15 or 20 times a night,” he said. “It got horrendous. I just couldn’t lie down.”
Rowland took six weeks off from work. However, when he spoke to his doctor again, “He said it’s anxiety and depression and put me on antidepressant medication. So, I tried this medication, and it made me even worse.”
Rowland’s doctor then prescribed “three or four” additional antidepressants, but none of them helped. Ultimately, his doctor said, “I don’t know what to do for you, I’m going to send you to a psychiatrist because I believe this is like a mental health [issue].”
“He didn’t think it was anything physical,” said Rowland, “and neither of us … I didn’t think it was a vaccine, because I had vaccines all my life. I didn’t figure it was the vaccine … no one put it down to the vaccine.”
Rowland eventually returned to work.
‘I just got sicker and sicker’
Whatever sense of normalcy Rowland reattained was short-lived. After receiving the second dose of the AstraZeneca vaccine, “That’s when all hell broke loose in my life.”
Rowland told The Defender:
“Immediately after having the second vaccine … I passed out once at work. I passed out at home … I developed chest pain immediately after the vaccine. I developed such chest pain and dizziness, and I was sweating. The pain was horrendous. I couldn’t breathe. I thought I was having a heart attack.”
Rowland was taken to the hospital, where he was told, “We can’t find anything wrong with you. We think it’s just a panic attack,” and he was sent home.
Not satisfied with the diagnosis, Rowland spoke to a cardiologist at his workplace and asked for an electrocardiogram (EKG or ECG). “So, he did a 24-hour ECG … and it basically showed my heart was going into ventricular tachycardia (VT), when I was getting all dizzy. It’s very dangerous and could cause sudden death.”
The cardiologist instructed Rowland to show the results of this exam to the hospital in the event he was to go back.
“Another week went by,” said Rowland, “I was getting tremendous pain and dizziness and I had another episode where I nearly collapsed again.” He showed paramedics the results of his ECG and was taken to the hospital.
But Rowland’s difficulties with doctors didn’t end there.
“I had a high D-dimer, so they started to look for blood clots on my lungs and kept me in hospital, wouldn’t let me move out of the bed.”
He added:
“They still didn’t think it was the vaccine when they couldn’t find blood clots … they sent my ECG to a specialist heart hospital … and got them to look at the ECG. Nobody thought it was the vaccine.”
As a result, Rowland was discharged and told he would be administered an MRI “in a couple of weeks,” with the expectation of finding cardiomyopathy. But the MRI didn’t find anything.
“Doctors were very, very confused about what was causing this VT,” he said. “They thought it was an adrenal problem and then referred me to an endocrinologist, and that’s when my horrible gaslighting and traumatic story really started. Because, again, they couldn’t find the cause of it, so they kept blaming things on anxiety.”
Rowland described what happened next:
“And then … I just got sicker and sicker. I developed blurred vision, face rashes, jaundice and tinnitus in my head. I started to develop neuropathy in my hands … some of my fingers don’t straighten anymore.
“I developed horrendous pain below both my knees … I can’t feel temperature in my lower legs. My toenails have died … I have no pulse in my feet.”
He was discharged from the hospital but returned monthly. Each time, doctors told him, “We can’t find what’s wrong with you.”
In June 2022, Rowland “collapsed with three pulmonary embolisms” in his lungs — but when he went to the hospital, they again told him it was just anxiety.
“So I said, ‘look at my eyes. I’ve lost two stone [one stone = 6.35 kilograms] in weight … I’m not leaving this hospital until you do some more scans and tests. This is definitely not anxiety.’”
So they scanned his lungs, and that’s when they found the three pulmonary embolisms and “a hundred tiny embolisms on my lungs.”
Rowland ended up in the hospital for a month, where he was diagnosed with pericarditis and told he would have died if they hadn’t found the embolisms.
Since then, Rowland said, “I’ve spent four more months in hospital on separate occasions. And I’ve been diagnosed now with severe thrombolytic vasculitis of my blood vessels.”
But that’s not all that’s wrong with his health. Rowland told The Defender:
“My diaphragm doesn’t work properly. Some of my eye muscles and my facial muscles aren’t working properly, and my leg muscles aren’t working properly … They did something called a CPET [cardiopulmonary exercise] test and … found that my cells in my muscles aren’t getting enough oxygen and nutrients.
“I’m waiting to see a vascular surgeon for the blood — it’s not getting to my legs and my muscles. I’m also waiting to see an immunologist and another hematologist because I’m on three blood-thinning medications and they don’t think it’s stopping my blood clotting properly.
“They think my blood is still clotting. They want me to have a special test where they take my blood out, spin it and take the platelets out and then look how my blood is responding to the three blood thinners I’m on, because for some reason it’s not doing its job.”
Rowland hasn’t been able to get that test because under the U.K. healthcare system, “the government won’t pay for it.”
He’s been trying to get the text through private healthcare. Meanwhile, his doctors tell him they can see that he’s really ill, “but we don’t know how to make it better” because they don’t know what’s in the vaccines. They suggested he travel to Germany to receive specialist treatment.
‘You’re the 239th person we have seen with similar symptoms from the vaccines’
Rowland described how he finally got a diagnosis that definitively linked the vaccine to his injuries:
“After I collapsed with the blood clots and they tried to send me home and I said ‘no, I’m not going anywhere, you scammed me, there’s something wrong,’ they finally admitted it was probably the vaccine.
“I was needing a wheelchair and they just discharged me and said, ‘Take this morphine, we’ll see you in four or five months’ time.’ And I was like, ‘I can’t even walk, you know?’ And they were like, ‘well, we can’t help you.’”
Rowland did his own research, locating a specialist hospital and private lung consultant, whom he visited in London, bringing with him the scans from the exams administered at his local hospital.
He said:
“I just said to him, ‘I feel like I’m dying, can you look at my scans and tell me, am I going to die, you know, imminently? I want you to be honest with me so I can tell my children.’ He looked at my scans and he said, ‘I don’t think you’re going to die imminently from your lungs’ … but he said to me, ‘it is 100% vaccine injury.’
“He said ‘you’re the 239th person we have seen with similar symptoms from the vaccines.’ And that was at one hospital in London … He said, ‘I’m more worried that you’re going to die with your heart and I need you to see one of my colleagues urgently.”
So Rowland saw a cardiologist who told him, it’s “completely vaccine injury. You don’t get VT like you developed for no reason. It’s definitely the vaccine with everything that’s happened to you since.’”
The doctor urged him to go to London immediately for treatment. “So they took me down to London for a month and then they diagnosed me … they realized it was in all my organs. So it’s in my heart, my lungs … so they diagnosed me with multisystem inflammatory syndrome.”
“So, at this moment in time, I’m on steroids for the pericarditis in my heart,” he said. “I’m on two different heart medications, another one for pericarditis [and] one for microvascular angina … and I’m on three blood thinners from my clotting, and various painkillers and things like that.”
‘It’s like living in hell’
As for what his life is like today, Rowland said:
“I don’t say these words slightly, but it’s like living in hell. It’s like torture, and I wouldn’t wish it on my worst enemy.”
He said he’s pretty much housebound and struggles to walk because of his breathing issues and chest pain.
Rowland added:
“Because I have fits trying to lie down, I can’t sleep in a regular bed … my bed’s adapted, so it’s at 45 degrees, so it’s like sitting up in a chair because the fits get triggered when I lie down.
“I don’t sleep. I just get these fits. So, every single day, I dread going to bed because the fits are so scary. And my heart sometimes misses a few beats and stops for a split second. And when I get that, it feels like I’m going to die.”
Rowland’s waking hours are not much better. He told The Defender:
“Because of my pain and my vulnerability, I can’t stand up for very long on some days. I struggle to make food. I can make breakfast and maybe lunch if I’m lucky, but I can’t cook myself an evening meal. When I go to the hospital, I never know whether I’m going to be able to walk from the car park to the hospital …
“Some days I can walk very short distances, 50 meters, maybe 100 meters. I’m really, really breathless … the chest pain is so bad that I can’t walk any further. And it does crazy things in my heart, it gives me the heart arrhythmia.”
Rowland also experiences blurred vision and struggles to type and write because of the neuropathy in his hands and because he can’t straighten some of his fingers.
Most days, he has to “live within the four walls of the house,” he said. “And then occasionally, when I’m on a good day, a friend might come and pick me up and take me for a drive to a nearby coffee shop and have a coffee. That’s about the most pleasure I’m getting in my life. I can’t walk my dog anymore. I can’t take my grandson to the park to push him on the swing.”
Rowland said he lost his wife and family because of the strain. “They couldn’t look after me,” he said. “I’ve not had a Christmas dinner with the family in two years because I’ve been too ill.”
As for his prognosis, Rowland said his doctors “don’t know how much I’ll heal or whether I’m just going to slowly die, because since I got injured, I’ve just gotten worse gradually on a linear projection.”
“I haven’t gotten any better,” he said, “so we don’t know what the future’s going to hold.”
‘I got to a point where I was suicidal’
The gaslighting Rowland experienced from multiple doctors, the lack of definitive answers, and the questioning of his mental health, drove him to the brink of suicide.
“Because they didn’t believe me … I felt like I was going crazy,” he said. “And I got to a point where I was suicidal.”
Rowland said many of the doctors he saw wanted him to be “on lots of pain medications: morphine, oxycontin, pregabalin.” He said his local hospital is “quite happy to give me morphine and all these other medications and leave me like that for the rest of my life.”
He doesn’t want to go back to taking lots of medications, he said, noting that morphine “doesn’t work … it takes a bit of the edge off the pain, but it doesn’t get rid of it.”
Rowland told The Defender he “wasn’t someone who watched TV or used social media.” But taking to social media ultimately helped provide Rowland with a new lease on life.
He said:
“I went on Twitter one evening. I don’t know what drew me to do that. This was when I was suicidal. I found a guy called Alex Mitchell in the U.K. who lost a leg [due to vaccine injury]. I started chatting to him and he was like, ‘it sounds like you might have a vaccine injury.’
“He pointed me to a support group, UK COVID Vaccine Family. I couldn’t believe it, that there was — I think at the time in the U.K. there were 600-odd people in this group — and I was like, ‘there’s all these people [with] all the same symptoms as me’ … It just completely opened my eyes.”
“From that moment,” said Rowland, while “it was nice to get the support, I still realized that the doctors didn’t have a clue what they were doing. I think what it did was, it took me from a place of being suicidal [to] where I wanted to fight for my life now.”
Rowland said he started to seek out specialists who were seeing patients with vaccine injuries and “knew it wasn’t all in their heads and knew what sort of tests to do.”
He also “went on Twitter and decided that I needed to speak out, because I thought, ‘well, if I’m going to die’ — and I didn’t realize how bad my story was — I thought, ‘well, I didn’t want anyone else to go through what I’m going through.’”
“I just wanted to warn people that if they do inject you and it goes wrong,” he said, “they tell you it’s safe and effective but there’s nobody there for you to help you.”
He said he’s met some wonderful people “who’ve reached out to me and offered me support.”
“I just take pleasure from speaking to those people and the people who are trying to help me,” said Rowland.
At the same time, Rowland told The Defender he is also “going down a legal route.”
“I want to know … what’s keeping my blood clotting and giving me vasculitis. [Doctors] don’t seem prepared to do that. So that’s the battle I’m on … I want to prove it’s negligence because then the [U.K.] government will have to pay for private treatment for me, even if it’s abroad. So, it’s about keeping me alive,” he said.
He had some words of advice for other vaccine-injured individuals:
“I think the first thing they need to do is, don’t suffer in silence alone … trust your own body and your intuition. So, if people are saying that to you, don’t just accept that if your intuition says otherwise.
“Try a two-pronged approach. Find a support group and question people in that support group. Even reach out and contact me online. That’s what I’m there for. And then also, if your doctor is gaslighting you … print off a lot of evidence. If your doctor is not helping you, you need to find another doctor, which I know is not as easy as that, but do not accept a doctor that’s telling you it’s in your head.”
Rowland encouraged vaccine injury victims to “come out publicly if you’ve got the strength to do that because there’s hundreds of thousands and probably millions of us around the world.”
“We were part of the worst experiment that I believe has probably ever taken place,” said Rowland. “And I think it’s going to be like a dam that’s going to burst by the back end of 2023 … I don’t think they can keep it covered up much longer.” (Exclusive: From the Peak of Fitness to Wanting to Die — How the COVID Vaccine Ruined One Man’s Life’s.)
Los Angeles County Sheriff’s officials confirmed that a detective was killed in a car crash on his way home from work near Torrance late on Sunday, January 15, after suffering a medical emergency.
Steven J. Lim, a detective and 26-year veteran of the LASD who “handled the most severe child abuse cases,” was identified as the victim of the single-car crash.
“It is with our most profound sorrow that we announce the sudden loss of a family member, Steven J. Lim, a Special Victim Bureau detective and 26-year veteran of LASD,” Los Angeles County Sheriff Robert Luna said in a statement.
“He was involved in a fatal traffic collision earlier today while driving home from his work assignment. He was an exemplary detective who handled the most severe child abuse cases,” he continued.
The cause of death was unclear but the Sheriff’s office said Lim had a medical emergency while driving home from work. (L.A. County Sheriff's Deputy Dies After Suffering Medical Emergency While Driving,)
Additionally, news came to light on Saturday, Feburary 25, 2023, that a twenty-five year-old Canadian medical student died suddenly because he was forced to get vaccinated as a condition of attending his medical college:
Dr. Anthony Emanuel Chifor grew up in Windsor, Ontario. His family, like mine, was from Slovakia and had emigrated to Canada to find a better life.
He graduated from University of Windsor where he was celebrated as an Outstanding Scholar and a Lead Gold Medallion Scholar, earning his B.Sc. in Biology and Biochemistry with Great Distinction and was part of the Dean’s Honour Roll.
He was studying medicine at Wayne State University School of Medicine, in Detroit Michigan (USA), when he was forced to take three COVID-19 vaccines to continue his medical training.
He was in the process of completing his 3rd year of medical school when he died suddenly at the age of 25, on January 17, 2023.
He is currently the youngest Canadian doctor death in my database.
According to my research, deaths of Canadian doctors under the age of 30 increased by 900% in 2022 compared to the 2019-2020 average.
His medical school continues to enforce its COVID-19 vaccine mandate. (Youngest Canadian doctor dies suddenly at age 25, was forced to take three COVID-19 vaccines by his Medical School. Also see Eric Clapton: "I can't sleep because of the pain...the vaccine took my immune system and just shook it around, Five Canadian teenagers ages 17-19 died suddenly in their sleep in the past month, and Canada's youngest athletes, ages 6-13 are dying suddenly: COVID-19 vaccine mandates for children playing sports were a crime.)
Anyone who can still religiously believe whatever a physician who subscribes the official vaccine narrative and who can ignore all this proof is a fool. It is a short step from the American Medical Association’s support for contraception, abortion, “brain death” and human vivisection, the starvation and dehydration of brain-damaged people, “hospice” and “palliative care” to most physicians putting their collective heads in the sand while “vaccine recipients” continue to die suddenly and others continue to be injured for life. Put not one’s total trust in any physician who lacks the moral and professional courage to break with the lies and to see reality for what it is.
Another person, a woman who lives in the State of Ohio, explained that she had never been healthier until receiving the vaccination as a condition of her employment. She developed traverse myelitis as a result:
Ohio native Danielle Baker had a career she loved, working as a certified hospice and palliative care registered nurse. She married the love of her life in the summer of 2020 and was enjoying life with her husband, her son and her stepdaughter.
By 2021, Baker was “the healthiest I had ever been,” she told The Defender.
But Baker’s life as she knew it came crashing to a halt, just days after being coerced in June 2021, by her then-employer, into receiving the two-dose series of the Pfizer-BioNTech COVID-19 vaccine.
Today, Baker, now 43, is permanently disabled, unable to work, faces financial ruin and has lost the ability to perform numerous everyday tasks and basic bodily functions.
In an interview with The Defender, following a separate interview with CHD.TV’s “The People’s Testament,” Baker shared her story.
Baker provided The Defender with extensive documentation and photographic evidence verifying her vaccination status, multiple diagnoses, including transverse myelitis, and current medical conditions.
{kind=link}
{kind=link}
‘We were so very active, always on the go’
Baker met her husband-to-be in 2019, at the same assisted living facility where she worked. By 2020, they were married and had blended their families.
Her son Ian, now 9, is “a kind-hearted high-functioning ADHD/autistic child.” Baker also welcomed into her life her husband’s daughter, Mady, now 10, “a beautiful girl with ADHD.”
“We were so very active, always on the go,” Baker said. “We felt important to expose our children to experiences in nature and did those adventures all the time, from primitive camping, hiking, hunting, fishing, canoeing — we really did do it all.”
Baker enjoyed her job as a certified hospice and palliative care registered nurse who worked on the frontlines during the first year-plus of the COVID-19 pandemic.
She described the difficulties of watching her patients suffer during COVID-19-related lockdowns and restrictions due to the lack of physical interaction with their families.
“I loved what I did,” said Baker. “I was afforded the honor to be invited into the homes [of my patients] and help those with limited time maintain autonomy and choose how they wanted their end-of-life care to look like.”
Baker had patients with life-limiting illnesses that progressed very rapidly and others that progressed over more time. “The one constant is the relationships I would build at the most vulnerable time,” she said. “I didn’t know it then, but God was teaching me the importance of the right to choose and maintaining autonomy.”
Baker always reviewed the “risks and benefits” when discussing medical treatment with her patients, and always allowed them to choose what they felt was in their best interests.
“My function wasn’t to have an opinion,” she said. “It was to present information and allow a path to be taken which was in line with that particular patient’s set of values. I had no trouble fighting for my patients and their medical rights.”
During COVID-19, her job became more difficult. “I watched too many lives suffer due to lack of family interaction because of the lockdowns, many times hearing from residents that ‘this fate is worse than death,’” said Baker.
‘Worst decision I ever made’
Baker came down with what she described as a mild case of COVID-19 in 2020. “The loss of taste and smell, along with fatigue, were the most bothersome of everything,” she said.
In the months that followed, she worked as usual but experienced “some brain fog” and “trouble thinking,” in addition to just feeling “off.” Despite these lingering symptoms, she continued to work.
Vaccine rollouts began in 2020-21 at her workplace. “The first to be vaccinated were healthcare workers and the elderly in facilities,” she said.
However, Baker described feeling “trepidation and hesitation, because I knew how the standards are for medication and getting it ‘passed’” through the regulatory agencies:
“I didn’t trust how fast it was zoomed through and that if you took the vaccine, you really had no idea what was going to happen. Add to it the [mRNA] technology being used, it was a perfect storm.
“In the cancer arena, gene therapy was getting traction … That in itself is worrisome to me. Taking a virus we know nothing about and then utilizing technology that allows it to penetrate down to the DNA? That was a big ‘no, I’m not getting it’ on my part.”
Baker said she’s always supported medical choice. “I wasn’t pro- or anti-vax, I was pro ‘let me have the information,’” she said. “But I had no plans to take it [the COVID-19 vaccine].”
During her CHD.TV interview, Baker said many of her co-workers felt similarly. “To know that they have this experimental — I hate even calling it a vaccine — experiment that they pushed through so fast and started jabbing people with it scared me to death,” she said, “And it scared most of our co-workers. And a lot of us didn’t want to take it.”
Baker was also confident she was protected because she already had the virus. “I developed COVID after a whole year of working in that environment without proper PPE, and I did just fine,” she said. “I came through it okay, and I know that gave me a natural immunity and I was okay with that.”
Baker said she was troubled that many of her patients disappeared after getting the vaccine:
“I remember when they started to do vaccinations in the nursing homes and assisted living [facilities], and people would load on a bus and go and they would have mass vaccinations.
“Thinking back, there would be empty rooms. These healthy people went for these vaccinations, and in a week or two, I saw their rooms were empty. I would ask the staff what happened, and a lot of times the answer was they had a stroke and died, or they had heart issues and had to move into a nursing home … I have no doubt that the shot is what escalated a lot of decline, even in our hospice patients.”
In spring 2021, her employer started sending emails to “encourage” staff to get the vaccine, pushing “the ‘safe and effective’ narrative” and offering incentives.
She said:
“An email came out stating we had until July to get the poison. If we didn’t take it and happened to acquire COVID, they would no longer pay for your days off. In addition, they put out a ‘safety net’ of sorts. The email stated that if you got the jab before July, then if you got sick because of the injection, you will be paid while off.”
Baker told CHD.TV her employer also offered other incentives, including cash bonuses of $100 and drawings for larger cash amounts, up to $5,000.
She also described “segregation” in the workplace, as unvaccinated staff members were required to be masked at all times. Employees were not informed about any possible exemptions.
“Our whole company knew the mandates were going to take effect in August [2021], so I took it with the belief in the ‘safety net,’” explained Baker.
She received the two-dose primary series of the Pfizer-BioNTech COVID-19 vaccine on June 4, 2021, and June 26, 2021.
{kind=link}
“I needed my career, I needed my income, I needed our insurance because I was the carrier,” Baker told CHD.TV. “Worst decision I ever made.”
Finally, a vaccine injury diagnosis
Baker’s adverse events started 18 days after she received her first dose. “I went to the ER feeling like I had a kidney stone, because the pain was that bad,” said Baker. “I was released with a muscle strain diagnosis.”
At first, she didn’t connect her symptoms with the injection. But things got much worse after her second shot, she said.
“On the day of my second vaccination, I had a fall,” Baker said. “I was in excruciating pain from up the neck to down the arm, with shooting numbness and tingling.”
She thought she had broken her collarbone, but when she went back to the ER, doctors dismissed her.
“They had me in and out of there in a half hour, they took an X-ray and told us that everything was fine and sent us on our way,” she said.
The next day, she was back in the ER with even worse symptoms. Doctors did a CT scan on her neck and told her she had a separated AC joint.
But Baker’s symptoms worsened between June 28 and July 17, 2021. She felt “uncomfortable” and “didn’t seem to be healing right,” she said. By July 17, she was experiencing “horrible back pain again, had lost her ability to walk with any coordination, and felt “foggy and tired.” It was “the worst back pain I ever had,” she said.
“Over the next four days, I went from being normal to not being able to really even eat,” Baker told CHD.TV.
Then, after several visits to various doctors and a spate of tests, including spinal taps, an ER doctor diagnosed Baker with transverse myelitis, a neurological disorder involving inflammation of the spinal cord.
{kind=link}
Baker said her “core group” of doctors now includes a primary care physician, a neurologist, an alternative pain practitioner and a consulting allopathic physician.
“All of those doctors are on the same page about my condition and directly link it to the shot” as “other causes have been ruled out,” said Baker.
Baker reported her vaccine-related adverse events to the Vaccine Adverse Event Reporting System (VAERS) and to MedWatch on Aug. 4, 2021.
“My VAERS report disappeared and my MedWatch report was never acknowledged,” she said. “Nobody else filed one on my behalf that I am aware of.”
Baker to FDA: ‘Shame on every single one of you’
Baker investigated the batch numbers of the Pfizer-BioNTech vaccines she received, and found they were associated with a disproportionately high number of adverse reaction reports, injuries and deaths.
According to documentation she provided to The Defender, batch number EW0181 of the Pfizer-BioNTech vaccine was associated with 1,685 adverse reaction reports, 32 disabilities, 16 life-threatening illnesses and 14 deaths.
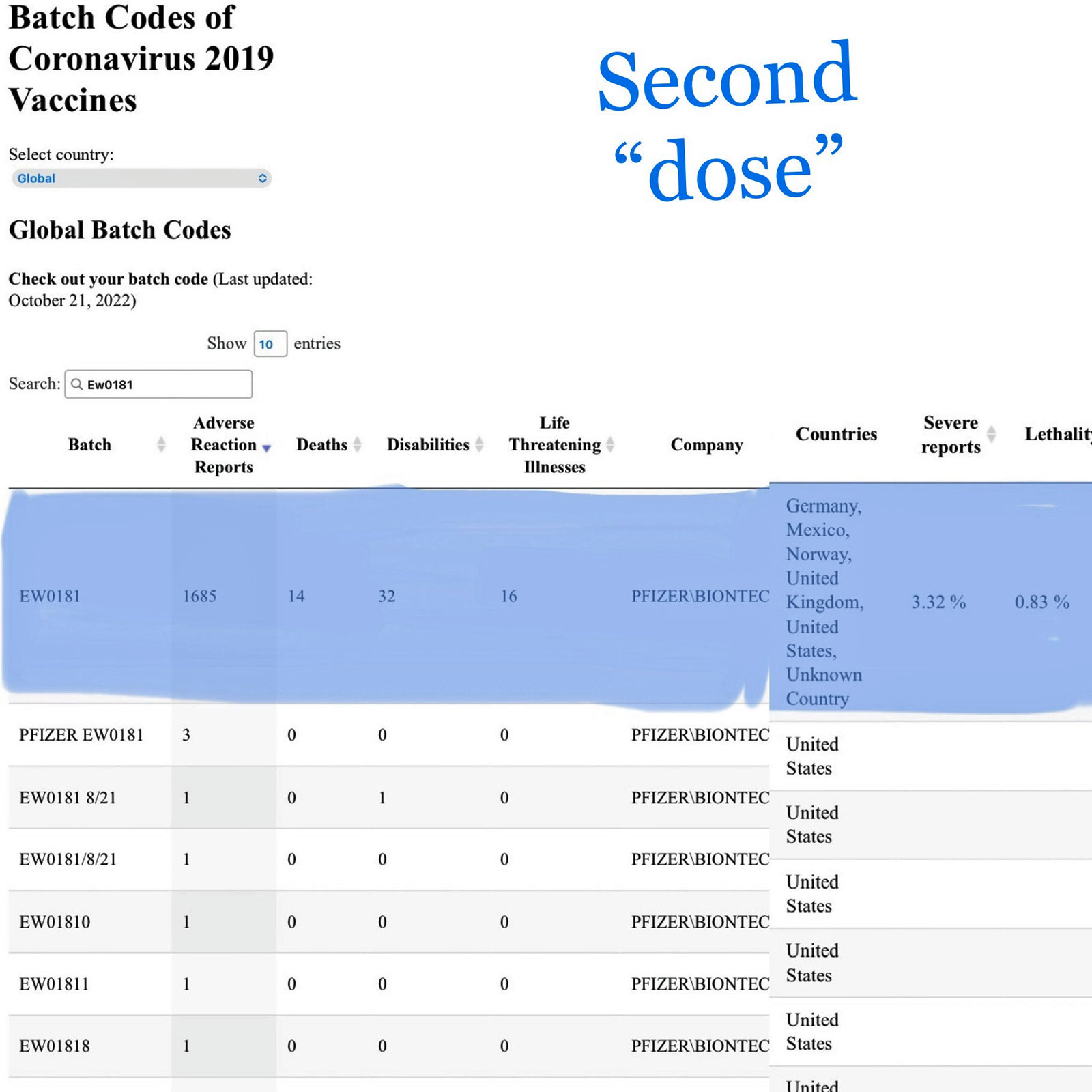{kind=link}
Thus far, 3.32% of individuals who received injections from this batch have reported severe adverse events, with a lethality of 0.83%.
Batch number EW0187 is associated with 1,757 adverse reactions, 24 disabilities, 31 life-threatening illnesses and 16 deaths. So far, 3.59% of those who received an injection from this batch reported severe adverse events, with a lethality of 0.91%.
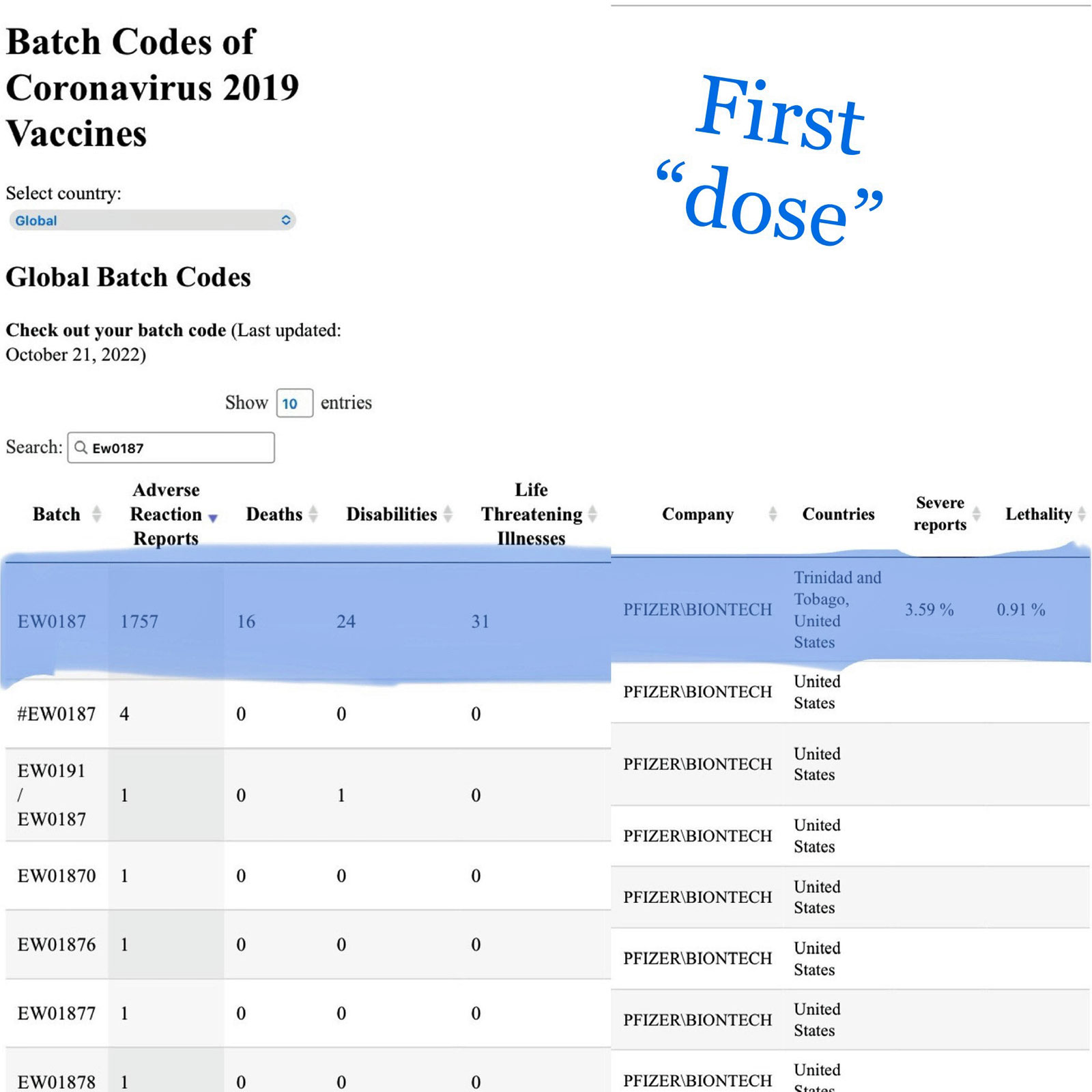{kind=link}
“Not only did I get one bad shot, I got two bad shots,” Baker said. “So, it explains why I am in the condition I am in.”
On Jan. 26, Baker provided a “heart-wrenching” victim impact statement to the U.S. Food and Drug Association (FDA), during a meeting of the agency’s Vaccines and Related Biological Products Advisory Committee.
Baker testified:
“The vaccine-injured are real. In June of 2021, I reluctantly received the Pfizer injection after being coerced by my former employer. I had a 17-year career as a certified and hospice palliative care registered nurse that I loved and was part of my identity.
“I asked if [my fall] was a direct result of the injection, but because of the ‘safe and effective’ narrative, I didn’t get the care that I needed and I was dismissed within 30 minutes without answers.
“We are in financial ruin because, ironically, I took the shot to keep the career that I loved and I no longer have.”
She concluded her testimony with scathing remarks for the FDA and other federal agencies:
“I submitted a VAERS report and a MedWatch in August 2021. My VAERS report disappeared from the system, and I have heard nothing from the FDA. Is it because you take your marching orders from Pfizer and Big Pharma? Will you continue to pretend I and the vaccine-injured don’t exist?
“The only thing more humiliating than losing my bodily function is your complete disregard for the vaccine-injured. Shame on every single one of you!”
Despite Baker’s testimony, FDA advisers voted that day to replace the original COVID-19 vaccine with bivalent boosters — despite a lack of clinical trial data.
As previously reported by The Defender, some advisory committee members have conflicts of interest with Big Pharma.
‘It puts a lot of strain on everybody’
Baker said she slowly regained function during the first three months after her injury, but it didn’t last.
“I am now completely disabled, unable to work as this has affected my physical capabilities along with my abilities to quickly and efficiently make decisions,” said Baker. “Even talking takes effort. I live day-to-day life in debilitating chronic pain.”
Baker still needs a walker or cane or scooter to move around and she’s in chronic pain. “Some days I can’t even tolerate human touch,” she said.
She added:
“I am chronically fatigued some days, with no energy to even move off the couch. My limbs turn cold, blue and painful on a regular basis. My heart rate drops below 50 often, and blood pressure skyrockets then plummets.
“I fall often, have bedsores and deal with chronic nausea, known to incapacitate me … My speech and cognition have both been affected and just putting words together is such a struggle.”
She can’t sleep in her bed “because by morning, my muscles have contracted and seized up, leaving me in tears.”
Baker’s condition also has affected her family, she said:
“My husband is now responsible for bringing an income in, transporting and taking care of the kids as well as taking care of me … To go anywhere means the need to pack up like you would for a child.
“It is hard to support the kids and their activities because I’m lucky to make it to their games, something I always took pride in attending.”
She’s “on so many medications just to help me get through the day,” she said. “It’s put a lot of strain on everybody, and they all tell me I’m not a burden, but I feel like I am and I’m stubborn.”
Help from support groups for the vaccine-injured and general public
Despite the challenges Baker faces on a daily basis and the hostile stance of her former employer toward her, Baker has found a high degree of support not just from her family, but from online support groups for vaccine-injured individuals, and from members of the general public.
Baker described the comfort she has found in interacting with other individuals with experiences such as herself, telling CHD.TV:
“My life aligned. I have my family and I have my close friends and I’m very thankful for that. But having an injured ‘family’ is different because they know exactly what you are going through. We all have similar problems and we’re able to talk about it and laugh about it to try to cope.
“I was so very fortunate when I was injured. I reached out and got connected into a wonderful group of people and it just grew from there. We remain united and we’ve found a purpose now, so that way we can be a voice to help all the other injured and spread the truth about this.”
Baker told The Defender that some of the groups she was able to connect to include the Vaccine Injury/Side Effects Support Group on Facebook, founded by another COVID-19 vaccine injury victim, Catherine “Cat” Parker, and Spirit PR, founded by Kevin Tuttle.
Describing her experience in these groups, Baker told The Defender “I have been blessed to have found a community of vaccine-injured and supporters. Knowing that there are people out there, such as yourself, fighting for us means more than I am able to articulate in words. They are my extended family now.”
Even this has not come without its challenges, however. For instance, Baker told The Defender that a video she uploaded to TikTok was censored and removed.
Baker has also found support from members of the general public, via contributions she has received as part of a fundraiser she has launched — funds which she says have helped her and her family get by.
“Just paying for day-to-day things is hard … The generosity of people is how we survive,” Baker told CHD.TV. “We wouldn’t be able to otherwise.”
This support has helped Baker find a new mission in life: to help others in similar situations as hers. “My mission is to attempt to help one person at a time through stepping up and sharing my story,” Baker told The Defender, “If I am able to accomplish that, then I have done what I am aiming to do.” (Exclusive: Woman Diagnosed With Vaccine-Induced Transverse Myelitis After Pfizer Shots.)
Julie Gamble had a fulfilling life: a stable career, the freedom to travel, and three children and one grandbaby to cherish.
But that life was disrupted in the spring and summer of 2021 when Gamble developed severe adverse reactions after getting the two-shot COVID-19 vaccine primary series — which resulted in her losing her job.
Gamble, now 53, spoke to The Defender about the vaccine injuries she sustained, the symptoms and challenges she is still experiencing, the ongoing difficulties finding doctors willing to treat her and classify her symptoms as vaccine-related, and the supportive role online groups for vaccine-injured individuals have had in her life.
The Defender reviewed documentation and photographic evidence verifying Gamble’s claims prior to publishing her story.
‘I felt really, really tired … anesthetic tired’
Gamble, who lives in Ontario, Canada, received the first dose of the Pfizer-BioNTech COVID-19 vaccine on May 17, 2021. For the second dose, she received the Moderna vaccine on July 18, 2021.
Her symptoms appeared almost immediately after the first dose, she said:
“I came home and I was really, really tired. It felt like an anesthetic tired, it didn’t feel like a ‘regular’ tired.
“I had developed a rash all over my body. I was itchy and my eyelids swelled up. I recall the bottoms of my feet being extremely itchy, more so than anywhere else, and I was sweating profusely. I started getting Charley horses in my calves. So, of course I was drinking a lot of water. I recall losing my vision in my right eye.”
Variations of the symptoms lasted for about a week after her first dose. She called a pharmacist who told her to take an antihistamine and, “if my tongue started to swell up, go to the ER.”
Soon afterward, Gamble developed other symptoms, including weakness in her ankles and a fluctuating heart rate.
“I also recall I was wearing my Fitbit. I’d walk into work, and I’d check my heart rate and sometimes it was at 140 and then it would drop down to regular, about 70 beats per minute. I’d be sitting down and I felt a little odd and I’d look at my Fitbit and my heart rate would shoot right up and then it would come right back down. And I stopped wearing it because I assumed my Fitbit was broken.”
The leg cramps kept getting worse, but Gamble attributed them to dehydration because where she worked “was quite hot, and so that’s what I thought was happening.”
‘I felt guilted’ into getting second dose
Gamble said her reactions to the Pfizer shot made her “leery” of getting a second dose — even her pharmacist recommended against it, she said.
“I spoke to the pharmacist about it, and I told him what had happened to me and about my muscles cramping up,” Gamble said. Her pharmacist recommended she see an immunologist before he would administer the second shot.
However, the doctor Gamble saw was far less sympathetic, she said:
“I didn’t have a family doctor, so I went down to the hospital thinking the receptionist or somebody would just book me an appointment with an immunologist.
“Instead, they put me in a waiting room. I saw a doctor and he told me right from the get-go he was not going to give me an exemption, he wasn’t going to give me an appointment with an immunologist. He told me to take an antihistamine and I would be fine.”
A combination of “nudging” from her doctor and Canada’s strict COVID-19-related restrictions led Gamble to go ahead with the second dose — especially after her doctor lectured her about “being a good citizen and not killing people,” she said.
“So, I felt guilted into it, and I knew I couldn’t leave Canada unless I was fully vaccinated.”
Gamble’s pharmacist was uncomfortable administering the second dose but proceeded on the doctor’s recommendation. Though Gamble didn’t develop a rash this time, she did experience fatigue and blurry vision again.
“I felt like, okay, I’m going to sleep this off. And once again, after about three days I started to feel a little bit better. But then I started dropping things all over the place. At first, I just kind of thought it was weird.
“But then I noticed my sense of perception was off. I’d go to open a door and where I thought the door was, my hand would be two inches away from the door. I started having brain zaps. I still tried to work, and so I was at work, and I tried to write a report and I could barely hold my pen. My hands were cramping up.”
Gamble also noticed slurred speech and changes in her ability to swallow food. “At that point, I decided obviously I can’t go to work. And I noticed muscles were starting to atrophy between my pinky finger and my ring finger.”
A neurologist at her local hospital, the London Health Sciences Centre in London, Ontario, “looked at my hands and said, ‘There’s something going on here.’” He admitted her for the night.
However, in the morning, another doctor dismissed her concerns, telling her she was ‘bending my arms too much.” She then made an appointment with a doctor she had seen during a previous adverse reaction to medication. But by that point, her condition had deteriorated further.
“I was losing the muscles rapidly,” Gamble said. “Within two months, I went from having normal-looking hands to completely skeleton-looking hands. The muscles in my arms started to atrophy, [and] in my feet behind my kneecaps. I could really feel it. My balance was off. My blood pressure was low.”
Trying to get a diagnosis ‘has been hell’
During one of several hospital visits, Gamble said doctors were particularly dishonest to her.
“One of the doctors said to me that some people are getting Guillain-Barré syndrome and he was going to check me for that. So, he gave me blood work.” But Gamble later learned that’s not even the right test for Guillain-Barré.
“They have to do it with a spinal tap,” she said. “I kind of feel like every doctor I saw had a reason to try to make up something different other than it was the vaccine.”
Gamble is still having trouble finding a doctor willing and able to treat her — and medication that will be effective and not cause further adverse reactions.
Meanwhile, she is dealing with multiple health-related challenges. “Just trying to get to the bottom of what is going on has been hell,” she said.
She has since found a family doctor who prescribed prednisone, but Gamble said she had a “horrible” reaction to it. “My hands turned blue, my tongue turned blue, I was getting brain zaps. I was passing out and my husband took me to the hospital.”
Doctors then told Gamble she had Raynaud’s disease, but “I don’t have that because [the symptoms were] on both sides of my hands and on my tongue,” she said.
She added:
“They sent me home like that. I tried to get help at one point, and I couldn’t get help. My husband, I guess I got a message out to him, but it was all gibberish. He came home thinking I’d had a stroke. He took me to the hospital; they did a CT scan, and everything came back normal. Apparently, my blood work comes back normal.”
Canada’s healthcare system, in conjunction with the country’s COVID-19-related restrictions, has made it challenging to even get treatment, Gamble said.
“I’m just trying to figure out what happened and am trying to get medical care,” Gamble said, “but I’m just hitting roadblocks everywhere. I figured maybe I could start physiotherapy, but in Canada you have to be 16 and under, or 65 and over, in order to qualify for free physiotherapy.”
Gamble said the pressure on doctors to look the other way when it comes to potential vaccine injury cases, and “a whole lot of doctor drama,” has been “frustrating.”
A neuromuscular doctor who previously worked at the London Health Sciences Centre confided in Gamble that she “got in trouble” with the Royal College of Physicians and Surgeons of Canada for writing COVID-19 vaccination exemptions. “And so, her hands are tied, pretty much,” Gamble said.
Meanwhile, Gamble’s symptoms continue to evolve, and doctors continue to reject the possibility that the vaccines are to blame. Recently, her tongue started “turning white and swelling up” and her ears became “really itchy and scabby.”
“My doctor thought this must be an allergy, so I went and I saw an immunologist,” she said. “But as soon as I showed him my hands and said, ‘vaccine,’ he told me he wasn’t interested in that. He was only interested in things that put you in instant anaphylactic shock.”
Gamble asked for a second appointment, during which it was noted that her heart rate had dropped to between 44 and 52 beats per minute. Doctors suggested she was experiencing a reaction to the prednisone.
Gamble asked to be tested for an allergy to polyethylene glycol, or PEG, because it’s unusual to have a reaction to prednisone, she said.
However, the response she got from her doctor was similar to the “gaslighting” reported by others who experienced vaccine injuries.
“The second doctor tested me and I said to him, since I’ve had this vaccine, I’m not doing well with certain foods or medications,” said Gamble. “And I talked to him about the muscle wasting, and he looked at my hands and he said he didn’t see it, which is ridiculous because it’s so obvious.”
Instead, the doctor “kind of wondered if it was psychosomatic,” said Gamble. She responded with, “no, I’ve had the nerve conduction studies done. It’s proven that my muscles are wasting.”
Gamble also saw a spine surgeon “who said she believes it’s a back injury.”
But one doctor Gamble saw later — a rheumatologist — was willing to draw a connection between her injuries and her vaccination.
“[The] rheumatologist said, ‘I don’t know what the big issue is. This is a vaccine injury.’ And she wrote me a letter to show people that I can’t be boosted.”
‘You kind of lose everything, don’t you?’
Unfortunately, Gamble said, Canada’s COVID-19 regulations restrict the extent to which exemptions are recognized.
Gamble told The Defender:
“I still can’t get a legal exemption, which is kind of important in a way because in Canada you can be refused a job. So, if I get better and I’m hoping I can go find employment again, they have the right to tell me that they’re not going to hire me because I’m not up to date on my booster. Or even traveling to another country — it’s up to them if they’re going to let me in if I’m not up to date on all this stuff.
“This government doesn’t seem to want to acknowledge the neurological damage. They only — from what I was told — give you an exemption if it’s a PEG allergy or if you have myocarditis, but not for neurological damage.”
As a result, said Gamble, “I’m going in circles here.” She described being told by a doctor that she “just happen[s] to be one of the people who ‘fall through the cracks’” — an obstacle that has also prevented her from collecting employment insurance.
She said:
“I don’t qualify for anything in my own country. And they have a vaccination injury support program, but very few people are getting paid out from that. It has to be ‘severe’ and it has to be permanent, and I don’t know if they’re going to consider this ‘severe,’ but right now I can’t work because I have no muscles left in my hands.”
Gamble did get severance pay, she said, but everything else “has been denied, denied.”
“The government in Canada, they certainly aren’t doing anything for people who are injured by the vaccine,” Gamble said. “So, you kind of lose everything, don’t you? And then you’re put in this category that you never wanted to be a part of.”
Despite these challenges and obstacles, Gamble perseveres, even though she can’t work.
“There are things that I want to do,” she said. “I want to start exercising, but I’m even scared of that because you see these videos [of people who] died suddenly … a lot of people apparently have died while they’ve been playing sports. So that’s a little bit concerning for me, and just in general, just still not knowing what happened to me.”
Online support groups for vaccine-injured individuals ‘a godsend’
In contrast to her experience with most doctors and many friends, who dismissed her condition, Gamble praised the support she’s received from members of online support groups for vaccine-injured individuals.
“It’s been a godsend,” she said. “For the first seven or eight months, I’m on my couch and I’m feeling my muscles wasting and I’m struggling to walk. Anybody that I tried to talk to that didn’t have an injury, they assumed it had to be something else, because they’ve been told that these vaccines are ‘safe and effective.’”
But participation in online groups, such as the Vaccine Injury/Side Effects Support Group on Facebook, has allowed Gamble to interact with “decent” people who “don’t judge” and who have experienced similar symptoms and conditions as her.
“I have found a few women with the exact same injuries that I have,” she said. “It was nice to know that there are other people out there, that you’re not alone. We don’t all share the same symptoms, but we share a lot of similar symptoms, and so I can say, ‘so-and-so tried this, well I’m going to try it.’”
Gamble said she’s not sure the medical system will ever regain her trust. But she had some advice for others experiencing vaccine injuries.
“People need to realize if they get injured by this vaccine, probably medically they’re not going to get a lot of help or [doctors] are going to try to tell them it wasn’t the vaccine.” (Exclusive: 53-Year-Old Woman Details Aftermath of COVID Vaccine Injury.)
Taking nothing away from the suffering of the three people who stories were recounted on the Children’s Health Defense website, it is nevertheless a telling commentary that none of these three victims knows anything about the theology of redemptive suffering, which would teach them that, although their suffering is real and was totally unavoidable, has occurred within the Providence of God, Who alone stands ready to provide them with the supernatural support that they need from the treasury of graces won for us by His Co-Equal, Co-Eternal Divine Son during His Redemptive Act on the wood of the Holy Cross on Good Friday. Nothing we suffer in this passing, mortal vale of tears is the equal of what one of our least Venial Sins caused Our Lord to suffer during His Passion and Death, and we must consider it our privilege to suffer in reparation for our sins as we accept whatever slight merit that they might earn from the patient endurance of our suffering with love, joy, and gratitude as the consecrated slaves of Our Blessed Lord and Saviour Jesus Christ through the Sorrowful and Immaculate Heart of Mary.
It is nothing other than tragic that the revolutions of Protestantism and Modernism have robbed most, including most Catholics, of any sense of the beauty and the privilege of suffering, especially if it has been imposed upon us unjustly by the misrepresentations of others as our we must remember that our sins imposed the greatest injustice of all: the death of the God-Man in ignominy on the dung heap of Golgotha, Mount Calvary. Those who do not understand this will, obviously, look to mere mortals for consolation in time of suffering, and although there is nothing inherently wrong in seeking the advice of others it is far more important for those who suffer to learn how to do so with gratitude as they seek to warn others about how the sufferings were imposed upon them so that the vaccinators will not have more victims that will be crying out for Divine justice against them at the moment of their Particular Judgment.
Even some within the Federal bureaucracy know that the “vaccines” have killed injured many untold numbers of people and that the cases of myocarditis have increased exponentially in people of all ages as result, which is why the Federal Aviation Administration (FAA) has quietly changed the parameters of what constitutes an acceptable electrocardiogram (EKG) so that pilots who are suffering from myocarditis can continue to be certified as flight worthy:
A recent update to the Federal Aviation Administration’s (FAA) electrocardiogram (EKG) test limits for pilots has some aviation and medical experts questioning if the FAA’s move is concerned that COVID-19 vaccine injuries may be contributing to an ongoing shortage of pilots.
The FAA on Oct. 26, 2022, changed its Guide for Aviation Medical Examiners (AME), increasing the acceptable “PR interval” from 200 to 300 milliseconds — a 50% increase.
The PR interval — the time it takes for an electrical impulse to be transmitted from one part of the heart to another — is a key indicator of heart health.
The FAA did not publicly announce the revision and, according to Just the News, also has not disclosed the data used to justify the change.
US Freedom Flyers (USFF), an advocacy group opposed to COVID-19 vaccine mandates for pilots, detected the change last month, The Epoch Times reported.
The USFF and some vaccine safety advocates suggested the FAA revised the limits because airlines’ vaccine mandates, which some argued violated FAA regulations, resulted in a significant number of pilots sustaining adverse events.
The revelations surfaced amid claims the FAA did not investigate multiple cases of vaccine-injured pilots, including incidents where disaster nearly occurred, and that there is increasing demand for unvaccinated pilots.
Some critics called for FAA officials to resign, alleging the vaccines endangered the health of pilots and the public.
‘A lot of pilots and a lot of damage’
According to Just the News, federal agencies “are withholding the data behind recent decisions that relate or may relate to COVID-19 vaccines and severe adverse events.”
The FAA “raised the maximum so-called PR interval for first-degree atrioventricular [AV] block to 300 milliseconds, with no regard to age, on the list of ‘normal variants’ that don’t require deferment in the absence of ‘symptoms or AME concerns.’”
This means the FAA now considers more health conditions to be acceptable.
Steve Kirsch, founder of the Vaccine Safety Research Foundation, said the new range “accommodates people who have cardiac injury.”
Multiple pilots have come forward to report cardiac injury and other adverse effects following their COVID-19 vaccination, as previously reported by The Defender.
Josh Yoder, a commercial pilot and co-founder of USFF, told The Epoch Times he believes the FAA’s changes are “a ticking time bomb on a level like we’ve never seen,” and that they increase the odds that a pilot’s heart condition will go undetected, which increases the risk of an aviation disaster.
Kirsch called the changes “extraordinary,” adding, “They did it hoping nobody would notice.” He said the change is “a tacit admission from the U.S. government that the COVID vaccine has damaged the hearts of our pilots. Not just a few pilots. A lot of pilots and a lot of damage.”
The FAA disputed the claims — as did media “fact checkers.”
There is “no evidence of aircraft accidents or incapacitations caused by pilots suffering medical complications associated with COVID-19 vaccines,” the FAA told The Epoch Times.
But Kirsch and others said this is because the FAA never investigated those incidents.
The FAA also said, “When making changes to medical requirements and guidance, the FAA follows standard processes based on data and science.”
Yet the agency did not release the data used to make the revision, despite media requests, including from Tucker Carlson, host of Fox News “Tucker Carlson Tonight.”
In a statement to Just the News, the FAA claimed it followed “standard processes based on data and science” that allowed it to “safely raise the tolerance used to screen for a certain heart condition.”
Federal Air Surgeon Dr. Susan Northrup said the FAA has “seen no evidence” of vaccine injuries that led to “aircraft accidents or pilot incapacitations.”
The Associated Press, in a “fact check” said the FAA’s revision wasn’t prompted by adverse events among pilots following COVID-19 vaccination. The AP, citing the FAA, said, “This change was made in response to new scientific evidence” from the FAA’s “cardiology consultants.”
Cardiologists weigh in
In a Jan. 5 essay, cardiologist Thomas Levy, M.D., J.D., called the FAA’s new guideline “arguably a shocking one, as many pilots are in the same age range when heart attacks occur without any early symptoms but with a normal ECG — the ECG being the only mandatory heart-related test.”
“A fatal heart attack from very advanced coronary artery disease could occur 10 minutes after the normal ECG was recorded,” Levy added.
While a PR interval longer than 200 ms doesn’t prove, on its own, that there is a heart problem, it “shouldn’t be ignored,” Levy told The Epoch Times, and warrants additional testing, as the heart may “no longer [be] completely healthy, and the conduction rate is slowing down.”
A PR interval even slightly exceeding 200 ms “is clearly associated with arrhythmias in the future, pacemakers, and early death,” Levy said, adding that this is especially concerning in light of the increased prevalence of myocarditis in recent years, noting that the condition can contribute to a longer PR interval.
A sudden burst of adrenalin, such as one caused by a stressful in-flight situation, can bring this problem to light, said Levy, adding that myocarditis can strike suddenly and without prior warning signs.
Military flight surgeon Dr. Theresa Long, during an appearance on “Tucker Carlson Tonight,” said the new interval “does not improve safety.” She noted that unlike military pilots, who get EKGs annually regardless of age, commercial pilots receive one at age 35 and then annually starting at age 40.
Long told The Epoch Times cardiologists have always told her, “It would be negligent … to see a PR interval of 290 and do nothing.” Long said she was puzzled and concerned by the FAA’s new limit and that it was not typical for the agency to make such a change without citing specific evidence or studies.
Former FAA safety inspector Stephen Carbone called the new guidelines “nothing short of safety sacrilege” and an “assault on aviation safety,” adding, “I can’t highlight enough how dangerous this is and how irresponsible.”
Dr. Peter Chambers, a retired U.S. military special operations flight surgeon, said the new guidelines remove “the ‘safety zone’ that allows us to catch the problem early,” adding, “You’re not even allowed to ask the questions” about adverse health effects experienced by vaccinated pilots.
What’s behind pilot shortage?
Epidemiologist Dr. Andrew Bostom said the most likely explanation for the FAA’s change “is very benign and practical: the airlines are losing pilots by attrition.” Bostom didn’t attribute the attrition to pilot vaccine injuries, but others are making this connection.
Kirsch, for instance, wrote:
“I’ll take an educated guess as to why [the FAA] did that. I believe it is because they knew if they kept the original range, too many pilots would have to be grounded. That would be extremely problematic; commercial aviation in the U.S. would be severely disrupted.
“In other words, the COVID vaccine has seriously injured a lot of pilots and the FAA knows it and said nothing because that would tip off the country that the vaccines are unsafe. And you aren’t allowed to do that.”
Kirsch noted that the timing of the October 2022 change — two years after the onset of the pandemic — rules out COVID-19.
“October 2022 is late for COVID,” Kirsch said. “If it was due to COVID, it would have happened well before now. They can make changes every month.”
According to a July 2022 report by Oliver Wyman Insights, “an impending pilot shortage was on the horizon” in early 2021, and it is now materializing, due to an aging workforce and mandatory retirement age of 65, and “a wave of early retirements at the height of the pandemic,” though the report didn’t specify the reason for that.
Vaccine-injured former pilot Bob Snow confirmed for The Defender the growing shortage of pilots in the U.S., noting that “former military aviators are a traditional source of pilots for the airlines, but the military no longer produces pilots in large numbers, so there is now a shortfall.”
“The airline industry does not seem as attractive to the younger generation as with prior generations,” Snow added.
FAA not investigating pilot vaccine injuries
The FAA never imposed a vaccine mandate on pilots, but the agency did issue “guidance” for pilots to get vaccinated. Many airlines and employers did impose mandates.
FAA regulations prohibit pilots from taking non-FDA-approved medical products, such as those issued under an Emergency Use Authorization (EUA), but the FAA overlooked this rule when advising pilots to receive the COVID-19 vaccines — which were issued under an EUA.
The Defender has previously reported on adverse events sustained by multiple commercial, military and private pilots and by air traffic controllers, following their COVID-19 vaccination. Some pilots lost their jobs, some even lost their lives.
Snow, for instance, suffered a heart attack six minutes after landing his commercial flight and is currently unable to fly, while Cody Flint narrowly averted a crash of his own.
When Kirsch emailed Northrup last week, soon after the change in the FAA’s guidelines were known, and he later spoke with Northrup by phone. According to Kirsch, Northrup revealed that neither she, nor anyone else at the FAA, investigated incidents like Snow’s.
Kirsch wrote:
“At first I thought she was lying, but it turns out she was telling the truth. She’s seen no evidence because even though she admitted on the call that she knew about Bob Snow, nobody at the FAA ever bothered to call him. Ever!!! So they’ve never seen the evidence because they deliberately refused to look at the evidence!!”
Kirsch asked Northrup to provide the data the FAA used to justify the guidelines change, to investigate pilot vaccine injuries and to host a public roundtable to “discuss the ‘safe and effective’ narrative” regarding COVID-19 vaccines and pilot safety.
He also asked Northrup to respond to the Aug.1, 2022, revelation by author Alex Berenson, a former journalist with The New York Times, that the pilots’ union at a major U.S. air carrier internally reported a 300% rise in long-term disability claims among its mostly vaccinated members.
“If she doesn’t hold a roundtable,” wrote Kirsch in one blog post, “it will be further confirmation that the FAA is afraid to investigate the safety issues.”
Kirsch also publicly called on Northrup to resign, adding that “if she doesn’t, the FAA should fire her” as “she has put the lives of pilots, FAA employees, and the public at risk by her abject failure to investigate safety concerns associated with the COVID vaccines.”
Kirsch added:
“I know of people inside the FAA and pilots who have been killed or permanently disabled because they followed the FAA’s directive to be vaccinated. Susan has not called any of these people to investigate. Nobody from the FAA has. That is a dereliction of duty.”
Kirsch noted that Northrup’s husband, John Hyle, is a pilot who “refused to take the COVID vaccine due to safety concerns.”
Others expressed similar concerns about the FAA’s actions — or inaction. At the Jan. 21 Restore Freedom Rally in Orlando, Florida, Yoder said, “The FAA is not upset that they’re killing pilots. They’re upset that we caught them.”
On Jan. 22, Yoder tweeted:
Kirsch is planning a roundtable in collaboration with USFF, The Highwire and Sen. Ron Johnson (R-Wis.). Kirsch described it as “a public hearing where we will put all the pilot and FAA employee injuries in full public view, including what actions the FAA took to investigate each injury.” (Did COVID Vaccine Injuries Influence FAA’s Revision of EKG Test Limits .)
Two people who recently flew from Orlando, Florida, to Charlotte, North Carolina on American Airlines told me that they saw less than three pilots and several cabin attendants in full uniforms flying as passengers. One of the pilots clocked in each passenger cabin attendant on a tablet computer as though they were getting paid for the travel just in case they were "needed," shall we say.
Now, although I have not flown since October of 2019 and have flown only twice before that since 2007, I have flown enough over my seventy-one years of life to know that there are times when pilots and cabin attendants fly as passengers. That is not unusual. However, it is entirely possible the unusual number of pilots and cabin attendants abord the relatively short flight from Orlando to Charlotte might have had something to do with the Federal Aviation Administration’s alteration of its EKG test limits.
All of this having been noted, Dr. Peter McCullough believes that an antidote might have been found to reverse the effects of the spike protein contained in the mRNA-based “vaccines, which have killed so many untold numbers of people and injured countless others here and around the world:
Far and away the most common question I get from those who took one of the COVID-19 vaccines is: “how do I get this out of my body.” The mRNA and adenoviral DNA products were rolled out with no idea on how or when the body would ever breakdown the genetic code. The synthetic mRNA carried on lipid nanoparticles appears to be resistant to breakdown by human ribonucleases by design so the product would be long-lasting and produce the protein product of interest for a considerable time period. This would be an advantage for a normal human protein being replaced in a rare genetic deficiency state (e.g. alpha galactosidase in Fabry’s disease). However, it is a big problem when the protein is the pathogenic SARS-CoV-2 Spike. The adenoviral DNA (Janssen) should broken down by deoxyribonuclease, however this has not be exhaustively studied.
This leaves dissolution of Spike protein as a therapeutic goal for the vaccine injured. With the respiratory infection, Spike is processed and activated by cellular proteases including transmembrane serine protein 2 (TMPRSS2), cathepsin, and furin. With vaccination, these systems may be avoided by systemic administration and production of Spike protein within cells. As a result, the pathogenesis of vaccine injury syndromes is believed to be driven by accumulation of Spike protein in cells, tissues, and organs.
Nattokinase is an enzyme is produced by fermenting soybeans with bacteria Bacillus subtilis var. natto and has been available as an oral supplement. It degrades fibrinogen, factor VII, cytokines, and factor VIII and has been studied for its cardiovascular benefits. Out of all the available therapies I have used in my practice and among all the proposed detoxification agents, I believe nattokinase and related peptides hold the greatest promise for patients at this time.
Tanikawa et al examined the effect of nattokinase on the Spike protein of SARS-CoV-2. In the first experiment they demonstrated that Spike was degraded in a time and dose dependent manner in a cell lysate preparation that could be analogous to a vaccine recipient. The second experiment demonstrated that nattokinase degraded the Spike protein in SARS-CoV-2 infected cells. This reproduced a similar study done by Oba and colleagues in 2021.
Nattokinase is dosed in fibrinolytic units (FU) per gram and can vary according to purity. Kurosawa and colleagues have shown in humans that after a single oral dose of 2000 FU D-dimer concentrations at 6, and 8 hours, and blood fibrin/fibrinogen degradation products at 4 hours after administration elevated significantly (p < 0.05, respectively). Thus an empiric starting dose could be 2000 FU twice a day. Full pharmacokinetic and pharmacodynamic studies have not been completed, but several years of market use as an over-the-counter supplement suggests nattokinase is safe with the main caveat being excessive bleeding and cautions with concurrent antiplatelet and anticoagulant drugs.
Based on these findings, nattokinase and similar products such as serrapeptase should undergo well-funded, accelerated preclinical and clinical development programs. The issue at hand is the urgency of time, similar to that with SARS-CoV-2 infection and empiric early therapy. It will take up to 20 years to have a fully developed pharmaceutical profile to characterize the safety and efficacy of nattokinase in the treatment of vaccine injury and post-COVID syndromes. Large number of people are sick now and many believe empiric treatment is justified given sufficiently low risk of side effects and potentially high reward. My recommendation is to discuss this with your doctor or seek a specialist in holistic or naturopathic medicine who is experienced with the safety profile of nattokinase in a range of applications. (Dissolution of Spike Protein by Nattokinase.)
Such a treatment is indeed promising as large numbers of people around the world are suffering from the long-term effects of the poisoned jabs, each of which, of course, is derived immorally from the stem-cell lines of butchered babies.
III. Dehumanizing Human Beings by the Mask Mandates
The third part of the global genocide that has taken place during the plandemic in the past three years is the assassination of a human being’s individuality and personality caused by the demand by the global health care fascists that everyone, including children, most of whom were not at risk from dying from the Wuhan virus, was required to wear to enter public facilities. This robbing of human identity, which had absolutely nothing to do with genuine public health, calls to mind Pope Pius XI’s description of Communism:
10. Communism, moreover, strips man of his liberty, robs human personality of all its dignity, and removes all the moral restraints that check the eruptions of blind impulse. There is no recognition of any right of the individual in his relations to the collectivity; no natural right is accorded to human personality, which is a mere cog-wheel in the Communist system. In man’s relations with other individuals, besides, Communists hold the principle of absolute equality, rejecting all hierarchy and divinely-constituted authority, including the authority of parents. What men call authority and subordination is derived from the community as its first and only font. Nor is the individual granted any property rights over material goods or the means of production, for inasmuch as these are the source of further wealth, their possession would give one man power over another. Precisely on this score, all forms of private property must be eradicated, for they are at the origin of all economic enslavement .
11. Refusing to human life any sacred or spiritual character, such a doctrine logically makes of marriage and the family a purely artificial and civil institution, the outcome of a specific economic system. There exists no matrimonial bond of a juridico-moral nature that is not subject to the whim of the individual or of the collectivity. Naturally, therefore, the notion of an indissoluble marriage-tie is scouted. Communism is particularly characterized by the rejection of any link that binds woman to the family and the home, and her emancipation is proclaimed as a basic principle. She is withdrawn from the family and the care of her children, to be thrust instead into public life and collective production under the same conditions as man. The care of home and children then devolves upon the collectivity. Finally, the right of education is denied to parents, for it is conceived as the exclusive prerogative of the community, in whose name and by whose mandate alone parents may exercise this right.
12. What would be the condition of a human society based on such materialistic tenets? It would be a collectivity with no other hierarchy than that of the economic system. It would have only one mission: the production of material things by means of collective labor, so that the goods of this world might be enjoyed in a paradise where each would “give according to his powers” and would “receive according to his needs.” Communism recognizes in the collectivity the right, or rather, unlimited discretion, to draft individuals for the labor of the collectivity with no regard for their personal welfare; so that even violence could be legitimately exercised to dragoon the recalcitrant against their wills. In the Communistic commonwealth morality and law would be nothing but a derivation of the existing economic order, purely earthly in origin and unstable in character. In a word. the Communists claim to inaugurate a new era and a new civilization which is the result of blind evolutionary forces culminating in a humanity without God. (Pope Pius XI, Divini Redemptoris, March 19, 1937.)
Distracted by the farce that is and will always be electoral politics as two organized crime families of naturalism (one which is committed to the pursuit of a collectivist agenda while the other is committed simply to the pursuit of its own electoral success) and by the bread and circuses of the world, most people alive today do not realize, do not care or actually support the slow, gradual triumph, albeit temporary until the Triumph of the Immaculate Heart of Mary, of the collectivist/communist mentality in almost every aspect of social life today. This mentality has been proselytized in public and many Catholic elementary and secondary schools, in public, secular and most Catholic colleges and universities, in the fields of law, medicine, “entertainment” (included collegiate and professional athletics), the arts (including literature) and by what still goes by the name of “journalism” but is actually a tool of elitists committed to the obliteration of all concept of “bourgeois” morality and “individuality” in the service of the “global reset," which did not begin with the pladenmic’s Event 201 at the Hotel Saint Pierre in New York, New York, on Friday, October 18, 2019.
Having accustomed large numbers of people, including most of the members of the Supreme Court of the United States of America as presently constituted, around the world to accept the word of alleged “experts,” the elites in charge of shaping public perception of reality have reached the point where the career civil servants must be considered as “infallible” sources of truth on all subjects from whom there can be no legitimate dissent, disagreement, or even a rational exchange of convictions in public debate.
Despite the globalists’ best efforts to stigmatize and repress dissent from their “infallible” edicts and protocols, each of which has been “infallible” only in the sense that they have been infallibly and unfailingly wrong, independent reports are beginning to emerge that prove all claims by the supposed spokesmen for “science” have been not only wrong but harmful to human beings:
We now have the most authoritative estimate of the value provided by wearing masks during the pandemic: approximately zero. The most rigorous and extensive review of the scientific literature concludes that neither surgical masks nor N95 masks have been shown to make a difference in reducing the spread of Covid-19 and other respiratory illnesses.
This verdict ought to be the death knell for mask mandates, but that would require the Centers for Disease Control (CDC) and the rest of the public-health establishment to forsake “the science”—and unfortunately, these leaders and their acolytes in the media seem as determined as ever to ignore actual science. Before the pandemic, clinical trials repeatedly showed little or no benefit from wearing masks in preventing the spread of respiratory illnesses like flu and colds. That was why, in their pre-2020 plans for dealing with a viral pandemic, the World Health Organization, the CDC, and other national public-health agencies did not recommend masking the public. But once Covid-19 arrived, magical thinking prevailed. Officials ignored the previous findings and plans, instead touting crude and easily debunked studies purporting to show that masks worked.
The gold standard for medical evidence is the randomized clinical trial, and the gold standard for analyzing this evidence is Cochrane (formerly the Cochrane Collaboration), the world’s largest and most respected organization for evaluating health interventions. Funded by the National Institutes of Health and other nations’ health agencies, it’s an international network of reviewers, based in London, that has partnerships with the WHO and Wikipedia. Medical journals have hailed it for being “the best single resource for methodologic research” and for being “recognized worldwide as the highest standard in evidence-based healthcare.”
It has published a new Cochrane review of the literature on masks, including trials during the Covid-19 pandemic in hospitals and in community settings. The 15 trials compared outcomes of wearing of surgical masks versus wearing no masks, and also versus N95 masks. The review, conducted by a dozen researchers from six countries, concludes that wearing any kind of face covering “probably makes little or no difference” in reducing the spread of respiratory illness.
It may seem intuitive that masks must do something. But even if they do trap droplets from coughs or sneezes (the reason that surgeons wear masks), they still allow tiny viruses to spread by aerosol even when worn correctly—and it’s unrealistic to expect most people to do so. While a mask may keep out some pathogens, its inner surface can also trap concentrations of pathogens that are then breathed back into the lungs. Whatever theoretical benefits there might be, in clinical trials the benefits have turned out to be either illusory or offset by negative factors. Oxford’s Tom Jefferson, the lead author of the Cochrane review, summed up the real science on masks: “There is just no evidence that they make any difference. Full stop.”
This lack of evidence would be enough to keep any new drug or medical treatment from being approved—much less one whose purported benefits had not even been weighed against the harmful side effects. As the Cochrane reviewers disapprovingly note, few of the clinical trials of masks even bothered to collect data on the harmful effects on subjects. Most public-health officials and journalists have ignored the downsides, too, and social-media platforms have censored evidence of those harms. But there’s no doubt, from dozens of peer-reviewed studies, that masks cause social, psychological, and medical problems, including a constellation of maladies called “mask-induced exhaustion syndrome.”
Yet public-health officials, in violation of the first-do-no-harm principle, continue recommending or mandating masks without good evidence of their effectiveness or any pretense of cost-benefit analysis. Masks are still required in many hospitals and other institutions. Despite all the data showing that Covid-19 poses virtually no risk to healthy children, the CDC continues to recommend masking all students in communities where infection rates are rising. While the WHO advises against masks for children under six, and the European Union advises against them for students under 12, the CDC cruelly recommends masking everyone from age two on up.
The CDC’s director, Rochelle Walensky, remains determined to ignore the best research on masks, as she made clear in a congressional hearing earlier this month. “Our masking guidance doesn’t really change with time,” she said when asked how the new review from Cochrane would affect the agency’s policies. “This is an important study,” she conceded, “but the Cochrane review only includes randomized clinical trials, and, as you can imagine, many of the randomized clinical trials were for other respiratory viruses.”
It was a statement remarkable for its chutzpah as well as its scientific incoherence. One of the worst mistakes of the CDC and other lavishly funded federal agencies was the failure to conduct randomized clinical trials to determine whether their policies were effective. The Cochrane review had to rely on pandemic mask trials conducted in other countries—and now Walensky has the gall to complain that other countries didn’t do enough of the research that U.S. agencies shirked. She’s right that some of the trials involved other viruses, but why dismiss them as irrelevant to the coronavirus? And while one can always wish for more studies to include in a meta-analysis, that’s no excuse to ignore the best available evidence in favor of the shoddy science peddled by her agency to defend its policies.
Early in the pandemic, the CDC justified its newfound enthusiasm for masks in a press release hailing “the latest science” from a case study of a hair salon in Missouri. “Wearing a mask prevented the spread of infection from two hair stylists to their customers,” the CDC proclaimed, a preposterously sweeping conclusion to draw from a small observational study that lacked a control group and had other obvious limitations (most of the salon’s customers were never even tested for Covid). On national television, Walensky touted another study, of schools in Arizona, as proof that masks dramatically reduced the spread of Covid, but the study’s methodology was so clearly flawed—and the results so out of line with rigorous studies—that other Covid researchers dismissed it as “ridiculous” and “so unreliable that it probably should not have been entered into the public discourse.”
Instead of sponsoring—or at least heeding—clinical trials, the CDC kept searching for confirmation from less reliable research. It repeatedly cherry-picked observational data, crediting masks for a short-term reduction in Covid rates in some localities while ignoring contrary data from more systematic analyses, such as a study that tracked rates nationwide over the entire first year of the pandemic—and found that neither mask mandates nor mask usage correlated with infection rates.
Can anything persuade the maskaholics in the public-health establishment and the public to give up their obsession? Some researchers, echoing Walensky, concede that the Cochrane review is the gold standard but argue that the clinical trials so far haven’t been extensive enough to rule out the possibility that masks might do some good. But that vague possibility is no reason to force masks on people: a public-health intervention is supposed to be based on solid evidence, not wishful thinking.
In his book Unmasked: The Global Failure of COVID Mask Mandates, data analyst Ian Miller devotes an entire chapter to graphs exposing the CDC’s statistical malfeasance. He also prepared a graph for a previous City Journal article that is worth showing again, because it’s a visual confirmation—from nationwide data, not clinical trials—of the conclusions in the Cochrane review. The graph tracks the results of the natural experiment that occurred across the United States in the first two years of the pandemic, when mask mandates were imposed and lifted at various times in 39 states.
The black line on the graph shows the weekly rate of Covid cases in states with mask mandates that week, while the orange line shows the rate in states without mandates. As you can see, the trajectories are virtually identical, and if you add up all those numbers, the cumulative rates of Covid cases are virtually identical, too. So are the cumulative rates of Covid mortality (the mortality rate is actually a little lower in the states without mask mandates). Hundreds of millions of Americans dutifully covered their faces in the states with mandates, and the result was the same as in the clinical trials analyzed by Cochrane: the masks made no difference. (New Cochrane Study on Masks and Covid.)
Perhaps only third in line after the manyfold ways in which the global “healthcare” industry “(actually kills off living human beings (the chemical and surgical assassination of the innocent preborn, the use of the medical industry’s manufactured, money-making myth of “brain death” to vivisect living human beings for their vital bodily organs, the starvation and dehydration of brain-damaged persons, hospice/palliative care as the means to directly cause the death of those said to lack a “good” “quality of life” caused by being chronically or terminally ill, and euthanasia, the use of which is being expanded in Canada to include teenagers under certain conditions, suicide/assisted suicide/physician-assisted suicide), and vaccines, including those that have been sterilizing women of childbearing years in Africa for at least the last three decades—see Chronicling the Adversary's Global Takeover of the Healthcare Industry and Life, Death, and Truth: Under Attack by Medicine and Law), the murder of the human personality is one of the chief goals of the globalists associated with the World Health Organization and the World Economic Forum as people robbed of their individuality and who lack a firm foundation in the Catholic Faith are prime candidates to surrender to self-annihilation.
Meanwhile, another study indicates that the once ubiquitous face masks that are still being worn by many of the “vaxxed,” who are either fearful of a virus is not a mortal threat to their lives and/or desirous of making a political statement by doing so, have actually caused people to die as breathing in one’s own carbon dioxide all day long is not exactly a way to enhance one’s longevity:
Mask mandates caused higher COVID-19 death rates, according to the bombshell claims made in a new medical journal report analyzing fatality rates across the state of Kansas.
The observational study – “The Foegen Effect: A Mechanism by Which Facemasks Contribute to the COVID-19 Case Fatality Rate” – was published in Medicine in February 2022, authored by German doctor Zacharias Fögen.
The paper analyzed “whether mandatory mask use influenced the case fatality rate in Kansas” during the time period of August 1st, 2020 to October 15th. Kansas was used for comparison because the state allowed each of its 105 counties to decide whether or not to implement mask mandates, with 81 counties deciding against the measure.
“The most important finding from this study is that contrary to the accepted thought that fewer people are dying because infection rates are reduced by masks, this was not the case,” summarized the paper.
“Results from this study strongly suggest that mask mandates actually caused about 1.5 times the number of deaths or ∼50% more deaths compared to no mask mandates.”
The study also posited a potential reason for the disparity in risk ratio (RR) for dying from COVID-19:
“A rationale for the increased RR by mandating masks is probably that virions that enter or those coughed out in droplets are retained in the facemask tissue, and after quick evaporation of the droplets, hypercondensed droplets or pure virions (virions not inside a droplet) are re-inhaled from a very short distance during inspiration.”
Dubbed the “Foegen effect,” the theory suggests that COVID-19 “virions spread (because of their smaller size) deeper into the respiratory tract.”
“They bypass the bronchi and are inhaled deep into the alveoli, where they can cause pneumonia instead of bronchitis, which would be typical of a virus infection.”
“These findings suggest that mask use might pose a yet unknown threat to the user instead of protecting them, making mask mandates a debatable epidemiologic intervention,” concludes the paper.
The study follows another recently published analysis of international data showing the same relationship between COVID-19 and masks. (Mask Mandates Caused MORE COVID Deaths, Study Alleges.)
I am pleasantly surprised to see the mainstream German publication Die Welt openly asserting that clinical trials of the “Pfizer COVID vaccine” were rife with fraud. (paywall-free German language link, PDF with English translation) What a change!
Again, click here for the English version saved as a PDF file.
The article explains that Pfizer unblinded and removed numerous patients who suffered adverse events from the Covid vaccine trial. It also gives examples of Pfizer subjects whose deaths were covered up. One of the victims described by Die Welt is Pfizer subject C4591001 1162 11621327, whose story I unearthed in July of 2022.
WELT has documents according to which patient no. 11621327 was found dead in his apartment three days after the 2nd dose, apparently a stroke. Patient #11521497 died 20 days after vaccination, diagnosis of cardiac arrest. "According to the current state of science, these two cases would be assigned to the vaccination," says the Berlin pharmaceutical specialist Susanne Wagner, "especially since the US health authority CDC is currently investigating strokes in vaccinated people and it is known
As you remember, Pfizer’s investigators falsely ruled these deaths unrelated.
Die Welt also describes Argentine lawyer Augusto Roux, who remained alive, but whose sufferings were written off as “anxiety.”
Three weeks later, test candidate Roux received the second dose. He remained under observation for 40 minutes, then left the hospital feeling good. In the taxi home he felt uncomfortable, and later he had shortness of breath, burning chest pain, nausea and fever. His urine turned black like cola and he passed out. Three days later, Roux was in the Alemán Hospital, several PCR tests for Covid were negative. Senior physician Gisela di Stilio noted in the discharge report, which is available to WELT: "Adverse reaction to the coronavirus vaccine (high probability)". The computer tomograph had provided images of fluid in Roux's heart. A pericardial effusion.
Over the next few months, Roux lost 14 kilos, he had liver problems, and his heart sometimes beat irregularly. … The diagnosis for the symptoms after the second vaccination is very likely to be "pericarditis", inflammation of the heart. All of this fits exactly with a clinical picture that the Paul Ehrlich Institute also has in its list of “rare side effects” for mRNA vaccines.
Note how Die Welt sarcastically puts “rare side events” in quotes.
… He found amazing things there. His story, one might think, should appear in Pfizer's pivotal study papers, but it doesn't. The pharmaceutical company's papers say Roux informed the research team that he was hospitalized with pneumonia on both sides, following the initial report, which was classified as an "adverse event of toxicity level 1". That could have nothing to do with the vaccine, the file goes on to say, it is probably a Covid infection. Not a word that Roux had tested negative for Corona in several PCR tests.
The paper finds more cases of Pfizer fraud:
Almost at the same time as the Roux case, there must have been an incident in the Buenos Aires test center. In one fell swoop, the test management said goodbye to 53 subjects on August 31, 2020. The test candidates were "unblinded", which means they were informed about their vaccination status, a process that the Pfizer study protocol expressly only provides for "in emergencies". But there is nothing about it in the approval study. In protocol documents that are available to WELT, and which are actually not intended for the public, those responsible get caught up in contradictions. "
Pfizer Fraud Discussed in Mainstream Press.
While Die Welt does an excellent job at exposing Pfizer’s trial fraud, which the FDA wanted to hide for 75 years, most of what it discussed is not new to us. What is new is that mainstream newspapers are now discussing it.
Die Welt mentions that Pfizer’s contracts included a liability waiver even for Pfizer's negligence and for "fraud or bad faith on the part of Pfizer itself."
I expect this “fraud waiver” will be litigated furiously in many countries. In the United States, liability for certain misdeeds, such as fraud, cannot be waived in advance because it would “violate public policy” and encourage fraud. Thus, I expect Ed Dowd’s “fraud vitiates all contracts” doctrine to prevail legally in many localities.
A “General COVID Reckoning” Will Follow!
A question that many of us are asking is, “will there be trials.” A friend of this substack, Eugyppius, concludes with regret that “there will be no Corona reckoning in Germany.”
I am not an expert on German politics, but I would like to make a statement: in more than one country, though possibly not in Germany, there WILL be Corona reckoning. A mini-reckoning is already happening in Florida, which gives us a hint of the future.
The governor of Florida, Ron DeSantis, is a shrewd political operator who expects to benefit politically from defending the public from Covid vaccines.
I am optimistic that some reckoning and some punishments will happen. Consider this:
- Almost everyone was affected by Corona vaccinations. People were either vaccinated or discriminated against, with the extent of discrimination varying from country to country.
- [added a day later] A large fraction of vaccinated people were forced to vaccinate and are resentful of what happened to them.
- Covid vaccination harmed a significant fraction of vaccine recipients. The harms are numerous. A Thailand study found 29% of young males having subclinical heart damage, for example. I discussed, numerous times, immune system damage affecting vaccinated people who suffer Covid reinfections and endless other illnesses.
- While many vaccinated individuals do not realize that Covid vaccines affected them, they can be easily convinced that they are vaccine victims when presented with evidence.
- Many vaccinated people had multiple COVID infections. If nudged, they will see the apparent disconnect between promises and the ugly reality.
- Lawsuits against Big Pharma, and possibly against Google and Facebook, will, naturally, make many people consider whether they are also victims when financial compensation becomes a possibility.
- People understandably fear death, and the excess mortality we are experiencing worldwide should unsettle any person whose risk of death is heightened in a mysterious, unknowable way.
- Many political operators will realize they can build a career by being anti-Covid-vaccine and demanding retributions.
- There is a possibility of mass hysteria created around “will the Covid vaccine kill me,” which the above-mentioned political operators can turn to their advantage. While this has the potential of turning ugly, it is an important factor.
The most important determinant of how much “Corona reckoning” we will see is the future fate of humanity and the disturbing trends of excess mortality and infertility.
I want these trends to reverse and mortality and fertility to return to normal. Such a fortunate turn of events would necessitate only a moderately serious reckoning.
In the highly undesirable case of the general public's health trends taking a turn for the worse, stricter punishments against people who lied to us and forced the public to take the deadly experimental vaccines would be perfectly acceptable.
National laws may need to be revised to allow legal punishment of wrongdoers who participated in a novel global biomedical crime that harmed billions of humans. In plenty of precedents, crimes against humanity committed under the color of national laws were successfully prosecuted.
So… do you think at least one country will see any “Corona reckoning”? (German Press Discusses Pfizer Vaccine Trial Fraud. Will "Covid Reckoning" Follow?.)
No, not one.
Oh, sure, there will be individuals in legislative persons, such as United States Senator Ronald Johnson (R-Wisconsin), who may hold hearings now and again upon the fraud that has been perpetrated upon the people of the world, including here in the United States. However, those in legislative minorities at a time when a feeble, demented globalist/statist/ “woke” octogenarian is in the White House being propped up by Edith Bolling Gant Wilson (Jill Biden), can no little more than to hold sessions, such as one Johnson held in January of this year, to put various facts in the public record for those who have the intellectual curiosity to examine with dispassion:
U.S. Sen. Ron Johnson (R-Wis.) Wednesday led a roundtable discussion — “COVID-19 Vaccines: What They Are, How They Work and Possible Causes of Injuries” — to shed light on the current state of knowledge surrounding the vaccine and the path forward. Distinguished doctors and scientists who specialize in COVID-19 vaccine research and treatment joined Johnson. The story they told of corruption and mismanagement of the COVID-19 pandemic is a turning point for humanity.
Most of the people on the panel suffered loss of income, loss of status or loss of their jobs because they publicized truths about COVID-19 and COVID-19 policies that were anathema to the medical establishment and detrimental to pharmaceutical profits.
COVID-19 policy has been a crime against humanity, and underlying that crime has been a crime against science. Science is held in high public regard, even as the reputations of most other institutions have declined in recent decades.
The reputation of science is based on open debate and logical evaluation of evidence. Debate has been stifled by people with money and power, and those same people then claim to speak for “science.”
The public is gradually recognizing the enormity of this fraud. I fear that public support for science will crumble.
Sen. Johnson started the roundtable discussion by reminding us that promising drugs for early treatment of COVID-19 were made known to him by some of the people at Wednesday’s hearing already in the spring of 2020, and yet our government agencies were advising against their use, despite long and assuring safety records.
Liz Willner, who created a website to make the Centers for Disease Control and Prevention’s (CDC) vaccine safety data available in a more accessible format, explained that according to VAERS (Vaccine Adverse Event Reporting System) data, vaccine injuries increased 20-fold in 2021 and vaccine-related deaths increased 50-fold.
Aaron Siri, a lawyer for Del Bigtree’s Informed Consent Action Network, described how the CDC created a system called V-Safe for recording a large sample of vaccine safety data, and then hid the data from the public.
Siri pressed through the Freedom of Information Act to obtain that data for more than one-and-a-half years before some of it was released. Much still remains secret.
Risk of myocarditis, Guillain-Barré syndrome, and autoimmune disorders was recognized and reported early in the Pfizer trials, and these conditions were in early specifications for the V-Safe system. In the end, none of these conditions were included, suggesting that CDC made a deliberate decision not to create a paper trail for them.
Ed Dowd, a securities analyst, reported data from Group Life Insurance policies that cover healthy, employed people ages 18 to 64. The death rate in this group jumped 40% in the third quarter of 2021, coincident with federal vaccine mandates for large employers who buy these Group Life Insurance policies.
The death rate for healthy, employed people is quite low, so the absolute number of deaths continued to be dominated by people who are old and sick. The overall death rate in America increased only a little during this time, but the Group Life Insurance companies took a big hit.
Josh Stirling, another security analyst, summarized data from Britain’s Office of National Statistics. To date, vaccinated people in the U.K. are dying at a rate 26% higher than the unvaccinated. The increase was concentrated in young people, who have suffered a 49% increased risk of mortality to date.
Lt. Col. Theresa Long, M.D., M.S. in public health, reported that alarming increases in disabling conditions for the U.S. Army were reported right after vaccination was mandated, and these signals were dismissed as a “computer glitch.”
The glitch was fixed, but disabling illnesses and injuries continue in the Army, where they are now occurring at almost twice the pre-vaccination rate of 2020. The number of military deaths from the COVID-19 vaccines is about 50% higher than the deaths from COVID-19 itself.
Dr. Ryan Cole reported that coronaviruses as a class mutate rapidly, and that’s why we have never had a vaccine for any coronavirus in the past. A largely vaccinated public drives the virus to mutate even faster. The current COVID-19 vaccines immunize against a variant of COVID-19 that was extinct more than a year ago.
Dr. Harvey Risch, Ph.D., emeritus professor of epidemiology from Yale, reminded us that for young, healthy people, the risk of serious COVID-19 is lower than the risk of injury from the COVID-19 vaccines.
Vaccine mandates can only be justified for vaccines that lower the risk of transmitting the virus, and the current vaccines do not prevent transmission, even in the old and vulnerable groups where they protect against serious COVID-19.
Dr. Pierre Kory specialized in pulmonary medicine and critical care as a professor at the University of Wisconsin before he was dismissed from its medical school for advocating early treatment for COVID-19.
He reminded us that early treatment has always been our best line of defense for everything from the common cold to cancer. (This includes the original SARS virus of 2003.)
Thirty percent of the world’s people live in countries where hydroxychloroquine or ivermectin is taken daily as preventives, and these countries have had much lower rates of COVID-19 mortality than the “developed world”, where these medicines were discouraged. Why were early treatments for COVID-19 disparaged by the authorities?
Dr. Paul Marik, with 300 peer-reviewed publications, is the second most published expert on critical care in the world. He estimated that hundreds of thousands of American deaths would have been avoided if hydroxychloroquine and ivermectin had been adopted as early treatments beginning in 2020.
He reported that in his hospital, he was forbidden from using safe, effective treatments for COVID-19, including vitamin C. Instead, he was encouraged to prescribe Remdesivir. Remdesivir is a patented antiviral drug and costs about $3,000 per patient.
But Remdesivir can only be administered in a hospital, and antivirals are useless by the time a patient gets to the hospital, because he is well past the stage where the virus has been vanquished, and the patient is threatened by its aftereffects, including lung damage, low blood oxygenation and sepsis.
Remdesivir is highly toxic to the kidney. According to the World Health Organization, Remdesivir increases the risk of kidney failure 20-fold. Marik claimed that there are no legitimate medical uses for Remdesivir, and yet federal reimbursement to hospitals is boosted by 20% (for the entire bill) if Remdesivir is included in the treatment plan.
Kory talked straight to doctors and medical researchers:
“High-impact journals have been under the control of the pharmaceutical industry. …
“We’ve seen repeated cases of manipulation of the data to show that a company’s product is effective and, conversely, manipulated trials to try to prove to everyone that safe, effective repurposed drugs that offered no profit were ineffective or dangerous.
“There is an immense amount of corruption in medical publishing and in the conduct of science.”
Dr. Peter McCullough, Ph.D., MPH, is a heart specialist with a Ph.D. in epidemiology, and was a professor at Baylor College of Medicine before he was dismissed for his vocal stance on early treatment of COVID-19. America suffered 250,000 deaths before the COVID-19 vaccines.
Normally, the second year of a pandemic is milder, both because the virus evolves to be less deadly and because the most vulnerable people were killed in the first year. But since the vaccine rollout, we have had 750,000 additional COVID-19 deaths in America. This is not the record of a successful vaccine.
Paul Alexander, Ph.D., reported that the COVID-19 vaccines lose their efficacy and dip into negative efficacy after a few months, such that people who have been vaccinated are more likely to get COVID-19 multiple times. Vaccinated individuals only have immunity to the part of the virus that is mutating most rapidly.
As long as we keep boosting people every few months, the virus will continue to mutate and the pandemic will continue for many more years. “Had we not mass vaccinated, it is probable that we would have achieved herd immunity in the United States in the winter of 2021.”
Dr. Robert Malone, who holds the patent as the original inventor of mRNA technology, changed his perspective on the COVID-19 vaccines after he had a near-fatal response to vaccination. Vaccine development is a very slow process, and viruses mutate rapidly.
The hope for mRNA technology was that a generic vaccine platform could be developed so that a new viral genome could just be plugged into an existing technology and vaccines could be developed at warp speed.
This very promising idea has not panned out, but those who are heavily invested in the paradigm refuse to recognize the failures and the danger of mRNA vaccine technology.
Malone described the innovation of using pseudouridine instead of natural uridine as one of the four nucleotide bases in mRNA vaccines. This is a trick that causes the body not to degrade mRNA as it normally would, so the mRNA stays around much longer.
The upshot is that once the body is injected with an mRNA vaccine, the mRNA stays around and continues to generate spike protein for at least 60 days.
We have no data beyond 60 days, so it is “at least” 60 days. The vaccine was designed to do its job of stimulating immunity in the first 48 hours. After this, the continued production of spike protein serves no protective purpose, but it can continue to be toxic.
Janci Lindsay, Ph.D., professor of toxicology, reported on the vaccines’ effects on fertility, and evidence that the mRNA can incorporate into the genome and be passed through sperm or egg to the next generation.
As long as the mRNA is turned into DNA, it can be passed to the next generation through plasmids in the sperm. The spike protein might become a part of the human genome.
David Wiseman, Ph.D., pharmacologist from Johnson & Johnson, told us that the U.S. Food and Drug Administration (FDA) has strict standards for safety testing of “vaccines” and much stricter standards for “gene therapies,” including 5 to 15 years of follow-up for cancer and DNA damage.
The FDA did not even apply the looser “vaccine” standards when evaluating the COVID-19 vaccines, even though these mRNA products meet the definition of “gene therapies.”
Cole reported on the change in definition of “vaccine” that made possible the approval of the mRNA products, which have a very different mechanism from traditional vaccines. They should have been tested with standards appropriate for gene therapies.
McCullough emphasized that immunity provided by the COVID-19 vaccines does not extend to the nose or throat, so that vaccinated people are exhaling a viral load that is no different from unvaccinated.
This is why the current crop of vaccines cannot stop transmission, and why any argument for mandating vaccination as a public health measure is flawed. “These vaccines have no support for reducing transmission of the infection.”
So the justification for vaccination must be lowering the risk of hospitalization and death. And yet, the only clinical trials that we had were not designed to measure rates of hospitalization and death.
NB Data from the Pfizer trial showed a higher death rate among the vaccinated compared to the control group.
Malone and Alexander raise the subject of “original antigenic sin.” In teaching the body to respond to just one part of the virus with one arm of the immune system, we hijack the body’s response when a COVID-19 virus comes along a few months later that has a mutated spike protein.
The immune system is fixated on the original spike protein, and its response to the altered virus is impaired. This is a well-known mechanism for several decades, so we should not be surprised when COVID-19 vaccines show negative effectiveness after a few months. (‘Crime Against Science’: Roundtable Discussion Exposes Government’s ‘Mismanagement’ of COVID Pandemic. Also see Cardiac Arrest and Death after COVID-19 Vaccination, Massive Clot Burden Days after Taking Janssen COVID-19 Vaccine, Inherited Risk of Sudden Death Triggered by COVID-19 Vaccination, UK gov’t admits COVID shots are ‘gene therapies,’ announces millions in funds for jab manufacturers, Inherited Risk of Sudden Death Triggered by COVID-19 Vaccination, Vaxxing, Covid, and International Mortality Rates and Unredacted NIH E-mails Show Efforts to Rule Out a Lab Origin of Covid.)
We are living through apocalyptic times. This does not mean that the “end is near.” However, it does mean that we are face to face with sociopathic monsters who want to mock the omnipotence and omniscience of God by remaking the world according to their own warped designs. Human beings are not only expendable in the eyes of these sociopathic monsters but they are to be considered as objects to be eliminated by the use of manufactured “pandemics” and “climate emergencies” that empower them to control and monitor the lives of everyone who escapes their genocidal schemes (see COVID was just the beginning: Climate lockdowns are the next stage of the Great Reset agenda).
Indeed, one of the reasons that the homosexual collective and their “woke” enablers are aggressively targeting innocent children to have their bodies mutilated into becoming something that they can never be, namely, the opposite gender, is to render boys and girls incapable of continuing the species. This all the inexorably result of the chemical and surgical execution of the innocent preborn, the breaking down of children’s natural psychological resistance to explicit material pertaining to the Sixth and Ninth Commandments, the feminist movement’s very successful efforts to destroy femininity by its leaders warfare against motherhood and to convince women to dress and act like men and to convince men to be effeminate and submissive to domineering women, and the proactive use of vaccines to sterilize women of childbearing years long before the plandemic of 2019-2020.
Indeed, a molecular biologist has warned very specifically that the mRNA “vaccines” could sterilize an entire generation:
WASHINGTON, D.C. (LifeSiteNews) — A toxicology expert with over 30 years of scientific experience issued a stark warning Wednesday about the potential reproductive harm she believes could be caused by the mRNA COVID jabs. She said more research is needed to determine the shots’ effects on reproduction.
In a Wednesday roundtable discussion hosted by U.S. Sen. Ron Johnson of Wisconsin, Dr. Janci Lindsay warned that the COVID-19 jabs could “potentially sterilize an entire generation” or else “be passed on to next generations as inadvertent gene transfer.”
Accordingly, Lindsay argued that it is “absolutely irresponsible to continue any of these shots” for children and people of child-bearing age “without investigating this,” explaining “there is no way that we can say at this point that they are safe nor effective.”
She ended her short address by calling for an investigation into the jabs’ potential danger to human reproduction.
Dr. Janci Lindsay holds a PhD in Biochemistry and Molecular Biology from the University of Texas Graduate School of Biomedical Sciences, and serves as the Director of Toxicology and Molecular Biology for consulting firm Toxicology Support Services, LLC. in Sealy, Texas.
According to her company’s website, Lindsay boasts “extensive experience in analyzing the molecular profile of pharmacologic responses as they pertain to the dose/response relationship.” The medical professional has also conducted risk assessments and evaluated “the toxicological profile of a variety of consumer and industrial products,” according to her profile.
At the Wednesday discussion, where she was joined by the likes of Dr. Peter McCullough and Dr. Robert Malone, Lindsay said that the Pfizer and Moderna COVID shots don’t just stay in the arm at the injection site, but rather spread throughout the body.
“We were told initially that it would just stay in the arm, but it does not. It ends up being distributed throughout the entire body for both Moderna and Pfizer,” she said, adding the “caveat” that Moderna’s jab contents haven’t been found in the kidneys.
“Now, what are those tissues? The brain, the spleen, the endocrine glands, the bone marrow, the blood preferentially, the ovaries and the testes,” she continued. “Now, what happens when gene therapies get to the ovaries and the testes? Well, we just don’t know because unfortunately it hasn’t been adequately studied.”
According to Lindsay, the jabs have the “potential to cause immense reproductive harm and potentially sterilize an entire generation.”
“This has not been looked into and it must be looked into,” Lindsay said. “I am demanding now that this be investigated.”
Lindsay’s arguments pushing back against the prevailing narrative regarding COVID-19 shots have unsurprisingly been met with criticism. Health fact-check site HealthFeedback argued that Lindsay’s arguments were “inaccurate,” explaining that “COVID-19 vaccines aren’t gene therapy as they cannot modify human DNA,” and that “COVID-19 vaccines don’t cause any fertility problems in men or women.”
However, not all experts agree that the mRNA jabs are not actually gene therapies.
In September of last year, mRNA technology pioneer Dr. Malone argued that the use of mRNA in COVID jabs amounts to “gene therapy applied to vaccines”, and backed up the concerns of skeptics who he said “have a right to be wary about a new technology that is not well understood,” LifeSiteNews previously reported.
Meanwhile in October 2021, the president of Bayer’s Pharmaceuticals Division called the mRNA technology found in Pfizer and Moderna’s COVID shots a “cell and gene therapy”, and joked that without the appearance of the coronavirus the general public wouldn’t have rolled up their sleeves to take it.
“If we had surveyed two years ago in the public – ‘would you be willing to take a gene or cell therapy and inject it into your body?’ – we probably would have had a 95% refusal rate,” he said.
Moreover, some experts disagree with those who have waved away worries about the jabs’ potential impacts on human reproduction.
A recent study that found high rates of menstrual abnormalities post-vaccination has contributed to concerns about the jabs’ impact on the female reproductive system. In addition, a peer-reviewed study found a decline in male fertility in the months immediately following reception of Pfizer’s mRNA COVID shot.
In February, a Swedish study suggested mRNA technology could potentially be integrated into DNA in cells, contradicting the CDC’s assurance that the COVID jabs won’t modify DNA.
In November, board-certified obstetrician-gynecologist and maternal fetal medicine physician Dr. James A. Thorp called the rollout of the COVID jabs for pregnant moms “the greatest disaster in the history of obstetrics and all of medicine.” (US medical group condemns chemical, surgical mutilation of the gender-confused.)
Yes, this has been a multi-faceted genocide of unprecedented proportions, staring with a genocide against truth, both supernatural and natural.
We must keep in mind the following words of Our Blessed Lord and Saviour Jesus Christ as recorded in the Gospel according to Saint Luke to help us to remain steadfast and without fear of any kind in this time when the forces of Modernity in the world and Modernism in the counterfeit church of conciliarism have combined to attack all that is holy and pure, starting with direct, frontal attacks upon Christ the King Himself and those who, despite their own sins and failings, try to be faithful to Him by following all that He has revealed to Holy Mother Church:
And when great multitudes stood about him, so that they trod one upon another, he began to say to his disciples: Beware ye of the leaven of the Pharisees, which is hypocrisy. 2 For there is nothing covered, that shall not be revealed: nor hidden, that shall not be known. 3 For whatsoever things you have spoken in darkness, shall be published in the light: and that which you have spoken in the ear in the chambers, shall be preached on the housetops. 4 And I say to you, my friends: Be not afraid of them who kill the body, and after that have no more that they can do. 5 But I will shew you whom you shall fear: fear ye him, who after he hath killed, hath power to cast into hell. Yea, I say to you, fear him. 6 Are not five sparrows sold for two farthings, and not one of them is forgotten before God? 7 Yea, the very hairs of your head are all numbered. Fear not therefore: you are of more value than many sparrows.
8 And I say to you, Whosoever shall confess me before men, him shall the Son of man also confess before the angels of God. 9 But he that shall deny me before men, shall be denied before the angels of God. 10 And whosoever speaketh a word against the Son of man, it shall be forgiven him: but to him that shall blaspheme against the Holy Ghost, it shall not be forgiven. 11 And when they shall bring you into the synagogues, and to magistrates and powers, be not solicitous how or what you shall answer, or what you shall say; 12 For the Holy Ghost shall teach you in the same hour what you must say.
13 And one of the multitude said to him: Master, speak to my brother that he divide the inheritance with me. 14 But he said to him: Man, who hath appointed me judge, or divider, over you? 15 And he said to them: Take heed and beware of all covetousness; for a man's life doth not consist in the abundance of things which he possesseth. (Luke 12: 1-15.)
We must pray to Our Lady to remain steadfast in the Holy Faith as well as praying very fervently for the conversion of the monsters who will one day have to render a reckoning to the very King of Kings whom they mock and revile.
IV. An Excuse for the Police State to Track the Unvaccinated
The fourth part of the ongoing genocide involves the insatiable appetite of the police state to find endless excuses to monitor the lives of ordinary people and to make sure that those who have refused the Wuhan virus jab get tracked and stigmatized for the rest of their earthly lives:
The U.S. government has secretly been tracking those who didn’t get the COVID jab, or are only partially jabbed, through a previously unknown surveillance program designed by the U.S. National Center for Health Statistics, a division of the Centers for Disease Control and Prevention.
- The program was implemented on April 1, 2022, and adopted by most medical clinics and hospitals across the U.S. until January 2023.
- Under this program, doctors at clinics and hospitals have been instructed to ask patients about their vaccination status, which is then added to their electronic medical records as a diagnostic code, known as the International Classification of Diseases, Tenth Revision (ICD-10) code, so that they can be tracked inside and outside of the medical system.
- These new ICD-10 codes are part of the government’s plan to implement medical tyranny using vaccine passports and digital IDs.
- They’re also tracking noncompliance with all other recommended vaccines using new ICD-10 codes, and have implemented codes to describe WHY you didn’t get a recommended vaccine. They’ve also added a billable ICD code for “vaccine safety counseling.”
As recently discovered and reported by Dr. Robert Malone, the U.S. government has secretly been tracking those who didn’t get the COVID jab, or are only partially jabbed, through a previously unknown surveillance program designed by the U.S. National Center for Health Statistics (NCHS), a division of the Centers for Disease Control and Prevention (CDC).
The program was implemented on April 1, 2022, but didn’t become universally adopted by most medical clinics and hospitals across the U.S. until January 2023.
Under this program, doctors at clinics and hospitals have been instructed to ask patients about their vaccination status, which is then added to their electronic medical records as a diagnostic code, known as the ICD-10 code, without their knowledge or consent so that they can be tracked — not just within the health care system but outside of it as well.
Secret tracking program revealed
The new ICD codes were introduced during the Sept. 14-15, 2021, ICD-10 Coordination and Maintenance Committee meeting. The ICD committee includes representatives from the Centers for Medicare and Medicaid Services and the NCHS.
According to the NCHS, “there is interest in being able to track people who are not immunized or only partially immunized,” and they figured out a way to do just that, by adding new ICD-10 codes.
As you can see below, ICD-10 code Z28.310 identifies those who have not received a COVID jab and Z28.311 identifies those who are not up-to-date on their shots.
Tracking unjabbed is part of the biosecurity agenda
Why do they want to track the unvaccinated? For what purpose? The short answer: to facilitate the implementation of vaccine passports.
As noted by Malone:
“Code Number Z28.310 listed above is not a code for an illness or diagnosis, but rather for non-compliance of a medical procedure … Once a person’s vaccination status is coded and uploaded into large data base, it can be accessed by government and private health insurers alike.
“The administrative state officers at the CDC have not made immunization status a reportable disease (yet) but immunization status is listed as one of the reasons for mandatory reporting. They are just one step away from being able to collect this information without your permission. Ergo: vaccine passports made easy. In this country, not having your vaccine records ‘up-to-date’ might mean:
The government will not restrict your travel, airlines will.
- The government will not restrict your travel, other nations will.
- The government will not restrict your travel, auto rental companies will.
- The government will not restrict your travel, public transport will.
- The government will not restrict your travel, private companies will.”
World Health Organization signed off on tracking codes
The ICD codes were created by the World Health Organization (WHO) and doctors — with the exception of those in private practice who don’t accept insurance — are required to use these codes to describe a patient’s condition and the care they received during their visit.
As noted by Malone, the fact that the ICD system is run by the WHO is an important detail, as this means the WHO had to authorize the CDC to add these new codes. The implication is that these codes may be in use internationally; we just don’t know it yet.
The codes are entered into your electronic health record and used by insurance companies for billing purposes. They’re also used by statisticians who track and analyze national and global disease trends such as cancer and heart disease rates over time.
Over the past decade, these statistical analyses have gotten easier to do, thanks to the transition into electronic record keeping. In the U.S., the ICD coding system has been fully integrated into the electronic health record system since 2012.
Within the ICD-10 codes, there’s a category called ICD-10-CM, and this is the category the CDC is now using to track the unvaccinated with specific codes for “Unvaccinated for COVID-19” and “Partially Vaccinated For COVID-19.”
Gross violation of medical privacy rights
Since there’s no billing or payment involved with being unvaccinated, and since being unvaccinated is extremely unlikely to be part of your disease profile, there’s no valid reason to record anyone’s vaccine refusal. It’s also a violation of medical privacy, as the records can be accessed by a variety of individuals and not just your personal doctors.
As noted by Malone, a person’s decision to get a vaccine or not is a private matter, and your privacy rights are enshrined in the Privacy Act of 1974. However, during the COVID pandemic, medical privacy rights have been repeatedly violated and broken.
Children’s vaccination statuses were shared with schools and employers were granted the “right” to know the jab status of their employees. Private venues were even permitted to demand proof of vaccination status — all this without a single word of the law having been revoked or amended.
They’re tracking reasons for jab refusal too
If you need proof that these codes will be used for reasons unrelated to your health, consider this: They’re also using codes to describe WHY you didn’t get the primary series or stopped getting boosters.
Those codes are listed in the screenshot below, under Z28.3 Underimmunization Status.

The use of “delinquent immunization status” under code Z28.39 also tells us something about where this is all headed. “Delinquent” means being “neglectful of a duty” or being “guilty of an offense.” Is refusing boosters a criminal offense? Perhaps not today, but someday, it probably will be.
All missed vaccinations will be tracked
Another tipoff that these codes are part and parcel of the biosecurity control grid is the fact that code Z28.39 — “Other underimmunization status” — is to be used “when a patient is not current on other, non-COVID vaccines.”
As detailed on the American Academy of Family Physicians website:
“The Centers for Disease Control and Prevention (CDC) and the Centers for Medicare & Medicaid Services have announced three new diagnosis codes, including two for COVID-19 immunization status …

“According to ICD-10-CM guidelines, clinicians may assign code Z28.310, ‘Unvaccinated for COVID-19,’ when the patient has not received a dose of any COVID-19 vaccine.
“Clinicians may assign code Z28.311, ‘Partially vaccinated for COVID-19,’ when the patient has received at least one dose of a multi-dose COVID-19 vaccine regimen, but has not received the doses necessary to meet the CDC definition of ‘fully vaccinated’ at the time of the encounter … New code Z28.39 is for reporting when a patient is not current on other, non-COVID vaccines.”
In other words, they have already begun tracking ALL of your vaccinations, not just the COVID shot, and they can use the Z28.3 sub-codes to identify why you refused a given vaccine.
Vaccine passports are a fait accompli — unless we act now
As noted by Malone:
“The administrative state is busy building a vaccine passport system that will be active before most Americans are aware of what is being done to them. No one is going to knock on your door asking for your vaccine status because they already know …
“They don’t need approval from Congress or the courts because we have given them the information through our health care providers. The CDC is the governmental organization tasked with tracking vaccine status on individuals.
“They already have the records, as well as updated booster information. They just need to tweak a definition here and there, or get President Biden to keep the COVID-19 public health emergency in place indefinitely and the vaccine passports will be a fait accompli.”
You can now be billed for immunization safety counseling
As if all of that weren’t tyrannical enough, they’ve also added a billable ICD-10 code for “immunization safety counseling.” That’s right. If you’ve decided you’re not willing to partake in the mRNA experiment, or you just don’t think you need some other vaccine that’s recommended, your doctor can bill your insurance for regurgitating the WHO’s vaccine propaganda.
This may become more or less automatic because, again, they have codes identifying whether you declined the COVID jab and/or any other vaccine, and for each vaccine refusal, there’s a code detailing why you declined it. “Belief or group pressure” is one of those, and you can bet that code, Z.28.1, will automatically qualify you for immunization safety counseling, whether you want it or not.
They also intend to indoctrinate your children and make you pay for it. The immunization safety counseling code, Z71.85, was described in the September 2021 issue of the American Academy of Pediatrics Pediatric Coding Newsletter.
You have to be a member to read the entire article, but here’s the publicly available preview:
“Reporting Encounters for Immunization Safety Counseling.
“As physicians and other qualified health care professionals field increasing numbers of concerns about immunization safety, International Classification of Diseases, 10th Revision, Clinical Modification(ICD-10-CM) offers a new code, Z71.85, for identifying immunization safety counseling as a reason for an encounter provided on or after October 1, 2021.
“Use this code when reporting counseling provided to patients and caregivers who are vaccine hesitant, wish to follow an alternative immunization schedule, or otherwise require time spent in counseling at lengths beyond that typical of routine immunization counseling.
“Code Z71.85 may be reported to indicate the principal or first-listed reason for an encounter or as a secondary reason.
“Documentation of time spent in preventive medicine counseling and separate time spent in immunization administration counseling should be explicit in the encounter note to support that the preventive medicine counseling was significant and separately identifiable.”
Unjabbed teachers flagged
In related news, in early February it was revealed that New York City teachers who did not get the jab were “flagged” with a “problem code” in their personnel files, triggering their fingerprints to be sent to the FBI and the New York Criminal Justice Services.
The purpose of this is unclear, but former public school teacher Michael Kane, founder of Teachers for Choice, believes “that unvaccinated NYC educators were being set up to be viewed as ‘right-wing extremists’ or even ‘terrorists.’”
Kane was among those who got fired for refusing the COVID jab. The revelation that teachers’ fingerprints were illegally entered into not just one, but two, criminal databases “are certain to open up a new round of lawsuits,” Kane writes.
Call to action
Knowing all of this, what can you do about it? How do we stop this madness? Here are a few suggestions:
1. Demand Congress finish what the Senate started by declaring the public health emergency over and done with. Jan. 17, 2023, HR 382, a bill “To terminate the public health emergency declared with respect to COVID-19” was referred to the House Committee on Energy and Commerce. This bill must be passed.
2. Contact your Congressional representative and let them know you:
- Support the Select Subcommittee on the Weaponization of the Federal Government’s investigation.
- Want Congress to reject all attempts by the administrative state, the U.N., the WHO, the U.S. Department of Health and Human Services and the Biden administration to require a vaccine passport or a digital ID.
- Expect them to work to ensure the freedom of travel for all citizens.
- Expect them to protect Constitutional rights.
- Expect them to protect all rights to privacy, including and especially medical privacy, and since these new ICD-10 codes are in violation of your right to privacy, you want them to take immediate action to ensure the codes are revoked.
With respect to what you can do to protect your medical privacy on a personal level, keep in mind that independent doctors are not required to use ICD codes unless they accept insurance. So, by choosing a doctor who is in private practice, you can avoid getting tagged and trapped in the system. (Here’s How the U.S. Government Is Tracking the Unvaccinated. I believe that the author made an error above as it is the Select Subcommittee on the Weaponization of the Federal Government is to be found in the United States House of Representatives, not the United States Senate.)
Obviously, our “smart phones” track us.
Every purchase we make online is tracked.
Our browsing history is tracked.
Surveillance cameras are everywhere for our own “protection,” of course.
Neighbors have been encouraged to spy upon each other to report the “non-compliant” to the appropriate civil authorities.
YouTube and PayPal accounts have been terminated without prior notice for the dissemination of what the Big Tech censors claim is “disinformation” of one sort or another.
In all this, however, we are not powerless as we have the power of Holy Mass, Our Lady’s Most Holy Rosary, the patronage of our beloved Saint Joseph and our Wonder Worker, Saint Philomena, and the constant intercession of all the angels and the saints. With such Heavenly assistance, you see, we have all the supernatural power we need to resist the wiles of the world, the flesh, and the devil, and we have all the graces necessary to prosper under temporal trials of this present moment, the very moment in salvation history that God has from all eternity appointed us to live in order to give Him honor and glory was we strive to sanctify and thus save our immortal souls as the consecrated slaves of His Divine Son, Our Blessed Lord and Saviour Jesus Christ, through the Sorrowful and Immaculate Heart of His Most Blessed Mother.
V. Concluding Remarks
Although I believed that I had mined all the information on this subject that could be useful to this site’s “vast” readership, which, evidently, consists of government monitors and the Christophobic employees of the Southern Poverty Law Center, when I posted part twelve of this series in 2021, it is unfortunately the case that new developments have required me to continue the series, which is why I am not going to say that this commentary is its last installment, noting that the frequency with which installments occur has slowed considerably.
Nonetheless, however, has been and continues to be my goal in all this to make information available to those who might not seek it out on their own so that they can pass it along to their own family members, friends, and associates.
Thus, it is important to emphasize the fact that remarkable turn of events in favor of totalitarianism has occurred, proximately speaking, because of the Protestant Revolution’s overthrow of the Social Reign of Christ the King that made possible the rise of the anti-Incarnational monster civil state of Modernity. Men who not believe that they will be account for their actions in this life will think nothing of lying and of plotting to kill and/or maim large numbers of people in this quest to build a antiseptically dystopian world where the “master class” gets to determine who lives and who dies and under what conditions those who live are permitted to exercise what have heretofore been considered the “freedoms” of the Western world. Totalitarianism must occur over the course of time when men and their nations do not submit themselves to Christ the King and to the authority of His true Church, the Catholic Church, in all that pertains to the good of souls.
In the final analysis, therefore, the terror and totalitarianism being used by our minders in the civil state should only fortify our resolve during this season of Lent to fear nothing other than Mortal Sin and the loss of our immortal souls for all eternity in hell. Our forefathers in the Faith suffered the likes of Nero, Domitian, Trajan, Diocletian, Julian the Apostate, various potentates of barbaric tribes and pagan peoples, Martin Luther, John Calvin, Henry VIII, Elizabeth I, Maximilian Robespierre, Napoleon Bonaparte, Giuseppe Garibaldi, Otto von Bismarck, Vladmir I. Lenin, Joseph Stalin, Ho Chi Minh, Mao Zedong, Pol Pot, and Fidel Castro. With the help of Our Lady’s graces, therefore, we can overcome the likes of Daniel Ortega, Xi Jinping, and the lords of the West in our own times.
The master of lies and the prince of darkness is the ultimate terrorist who seeks to impose a totalitarian control over our own interior lives, which is why Holy Mother Church gives us this holy season of penance, prayer, fasting, and almsgiving, Lent, as the means to build up our spiritual lives by refusing to be agitated by the events of a world gone mad because it is at war with Christ the King, His true Church and thus with both the spiritual and temporal good of the souls for whom Our King shed every drop of His Most Precious Blood to redeem.
Dom Prosper Gueranger’s reflection on the First Sunday of Lent, which is celebrated tomorrow, Sunday, February 26, 2023, reminds us that Our Blessed Lord and Saviour Jesus Christ underwent His temptations in the desert to show us that we, too, empowered by the ineffable graces He has won for us during His Passion and Death on the wood of the Holy Cross and that flow into our souls through the Sorrowful and Immaculate Heart of Mary, can overcome the devil, his pomps and his empty works, including everything to with worldly and fleshly desires:
Lent solemnly opens today. We have already noticed that the four preceding days were added since the time of Gregory the Great, in order to make up Forty days of fasting. Neither can we look upon Ash Wednesday as the solemn opening of the Season, for the Faithful are not bound to hear Mass on that day. The Holy Church, seeing her children now assembled together, speaks to them, in her Office of Matins, these eloquent and noble words of St. Leo the Great: “Having to announce to you, dearly beloved, the most sacred and chief Fast, how can I more appropriately begin, than with the words of the Apostle (in whom Christ himself spoke), and by saying to you what has just been read: Behold! now is the acceptable time; behold! now is the day of salvation. For although there be no time which is not replete with divine gifts, and we may always, by God’s grace, have access to his mercy—yet ought we all to redouble our efforts to make spiritual progress and be animated with unusual confidence now that the anniversary of the day of our Redemption is approaching, inviting us to devote ourselves to every good work, that so we may celebrate, with purity of body and mind, the incomparable Mystery of our Lord’s Passion.
“It is true, that our devotion and reverence towards so great a Mystery should be kept up during the whole year, and we ourselves be, at all times, in the eyes of God, the same as we are bound to be at the Easter Solemnity. But this is an effort which only few among us have the courage to sustain. The weakness of the flesh induces us to relent our austerities; the various occupations of every-day life take up our thoughts; and thus, even the virtuous find their hearts clogged by this world’s dust. Hence it is, that our Lord has most providentially given us these Forty Days, whose holy exercises should be to us a remedy, whereby to regain our purity of soul. The good works and the holy fastings of this Season were instituted as an atonement and obliteration of the sins we commit during the rest of the Year.
“Now, therefore, that we are about to enter upon these days, which are so full of mystery, and were instituted for the holy purpose of purifying both our soul and body, let us, dearly beloved, be careful to do as the Apostle bids us, and cleanse ourselves from all defilement of the flesh and the spirit: that thus the combat between the two substances being made less fierce, the soul, which, when she herself is subject to God, ought to be the ruler of the body, will recover her own dignity and position. Let us also avoid giving offence to any man, so that there be none to blame or speak evil things of us. For we deserve the harsh remarks of infidels, and we provoke the tongues of the wicked to blaspheme religion, when we, who fast, lead unholy lives. For our Fast does not consist in the mere abstaining from food; nor is it of much use to deny food to our body, unless we restrain the soul from sin.” [Fourth Sermon for Lent]
Each Sunday of Lent offers to our consideration a passage from the Gospel, which is in keeping with the sentiments wherewith the Church would have us be filled. To-day she brings before us the Temptation of our Lord in the Desert. What light and encouragement there is for us in this instruction!
We acknowledge ourselves to be sinners; we are engaged, at this very time, in doing penance for the sins we have committed;- but, how was it that we fell into sin? The devil tempted us; we did not reject the temptation; then, we yielded to the suggestion, and the sin was committed. This is the history of our past; and such it would, also, be for the future, were we not to profit by the lesson given us, to-day, by our Redeemer.
When the Apostle speaks of the wonderful mercy shown us by our Divine Savior, who vouchsafed to make himself like to us in all things, save in sin, he justly lays stress on his temptations. He who was very God, humbled himself even so low as this, to prove how tenderly he compassionated us. Here, then, we have the Saint of Saints allowing the wicked spirit to approach him, in order that we might learn from His example how we are to gain victory under temptation.
Satan has had his eye upon Jesus; he is troubled at beholding such matchless virtue. The wonderful circumstances of his Birth—the Shepherds called by Angels to his Crib, and the Magi guided by the Star; the Infant’s escape from Herod’s plot; the testimony rendered to this new Prophet by John the Baptist—all these things which seem so out of keeping with the thirty years spent in obscurity at Nazareth are a mystery to the infernal serpent, and fill him with apprehension. The ineffable mystery of the Incarnation has been accomplished unknown to him; he never once suspects that the humble Virgin, Mary, is she who was foretold by the Prophet Isaias, as having to bring forth the Emmanuel; but he is aware that the time is to come, that the last Week spoken of to Daniel has begun its course, and that the very Pagans are looking towards Judea for a Deliverer. He is afraid of this Jesus; he resolves to speak with him, and elicit from him some expression which will show him whether he be or not the Son of God; he will tempt him to some imperfection, or sin, which, should he commit, will prove that the object of so much fear is, after all, but a mortal and sinful Man.
The enemy of God and men was, of course, disappointed. He approached Jesus; but all his efforts only turn to his own confusion. Our Redeemer, with all the self-possession and easy majesty of a God-Man, repels the attacks of Satan; but he reveals not his heavenly origin. The wicked spirit retires, without having made any discovery beyond this, – that Jesus is a prophet, faithful to God. Later on, when he sees the Son of God treated with contempt, calumniated, and persecuted; when he finds, that his own attempts to have him put to death, are so successful;- his pride and his blindness will be at their height: and not till Jesus expires on the Cross, will he learn, that his victim was not merely Man, but Man and God. Then will he discover, how all his plots against Jesus have but served to manifest, in all their beauty, the Mercy and Justice of God;- his Mercy, because be saved mankind: and his Justice, because be broke the power of hell for ever.
These were the designs of Divine Providence in permitting the wicked spirit to defile, by his presence, the retreat of Jesus, and speak to him, and lay his hands upon him. But, let us attentively consider the triple temptation in all its circumstances; for our Redeemer only suffered it, in order that he might instruct and encourage us.
We have three enemies to fight against; our soul has three dangers; for as the Beloved Disciple says: All that is in the world, is the concupiscence of the flesh, and the concupiscence of the eyes, and the pride of life! By the concupiscence of the flesh, is meant the love of sensual things, which covets whatever is agreeable to the flesh and, when not curbed, draws the soul into unlawful pleasures. Concupiscence of the eyes expresses the love of the goods of this world, such as riches, and possessions; these dazzle the eye, and then seduce the heart. Pride of life is that confidence in ourselves which leads us to be vain and presumptuous, and makes us forget that all we have—our life and our every good gift—we have from God.
Not one of our sins but what comes from one of these three sources; not one of our temptations but what aims at making us accept the concupiscence of the flesh, or the concupiscence of the eyes, or the pride of life. Our Saviour, then, who would be our model in all things, deigned to subject himself to these three temptations.
First of all, Satan tempts him in what regards the Flesh:- he suggests to him to satisfy the cravings of hunger, by working a miracle, and changing the stones into bread. If Jesus consent, and show an eagerness in giving this indulgence to his body, the tempter will conclude that he is but a frail mortal, subject to concupiscence like other men. When he tempts us, who have inherited evil concupiscence from Adam, his suggestions go further than this; he endeavours to defile the soul by the body. But the sovereign holiness of the Incarnate Word could never permit Satan to use upon Him the power which he has received of tempting man in his outward senses. The lesson, therefore, which the Son of God here gives us, is one of temperance: but we know, that, for us, temperance is the mother of purity, and that intemperance excites our senses to rebel.
The second temptation is to pride; Cast thyself down; the Angels shall bear thee up in their hands. The enemy is anxious to see if the favours of heaven have produced in Jesus’ soul that haughtiness, that ungrateful self-confidence, which makes the creature arrogate God’s gifts to itself, and forget its benefactor. Here, also, he is foiled; our Redeemer’s humility confounds the pride of the rebel angel.
He then makes a last effort: he hopes to gain over by ambition Him who has given such proofs of temperance and humility. He shows him all the kingdoms of the world, and the glory of them; and says to him: All these will I give thee, if falling down, thou wilt adore me. Jesus rejects the wretched offer, and drives from him the seducer, the prince of this world; hereby teaching us that we must despise the riches of this world, as often as our keeping our getting them is to be on the condition of our violating the law of God and paying homage to Satan.
But, let us observe how it is, that our Divine Model, our Redeemer, overcomes the tempter. Does be hearken to his words? Does he allow the temptation time? and give it strength by delay? We did so, when we were tempted, and we fell. But our Lord immediately meets each temptation with the shield of God’s word. He says: It is written: Not on bread alone doth man live. – It is written: Thou shalt not tempt the Lord thy God. – It is written: The Lord thy God shalt thou adore, and Him only shalt thou serve. – This, then, must be our practice for the time to come. Eve brought perdition on herself, and on the whole human race, because she listened to the serpent. He that dallies with temptation, is sure to fall. We are now in a Season of extraordinary grace; our hearts are on the watch, dangerous occasions are removed, everything that savours of worldliness is laid aside; our souls, purified by prayer, fasting, and almsdeeds, are to rise with Christ, to a new life;- but, shall we persevere? All depends upon how we behave under temptation. Here, at the very opening of Lent, the Church gives us this passage of the Holy Gospel, that we may have, not only precept, but example. If we be attentive and faithful, the lesson she gives us will produce its fruit; and when we come to the Easter Solemnity, we shall have those sure pledges of perseverance, – vigilance, self-diffidence, prayer, and the never-failing help of Divine Grace. (Dom Prosper Gueranger, O.S.B., The Liturgical Year, First Sunday of Lent.)
Begging Our Lady for her help during these days of Lent, may we grow ever more reliant upon her Most Holy Rosary and thus ever more confident and joyful to carry whatever crosses we are asked to bear for the Kingdom of her Divine Son, Who suffered lovingly in obedience to His Co-Equal, Co-Eternal God the Father in Heaven and to make it possible for us, whom He loves from the depths of His Most Sacred Heart, to enjoy an unending Easter Sunday of glory in Paradise, where we will understand clearly that the Holy Cross of the Divine Redeemer is the one and only standard of true human liberty on earth and the one and only means by which we can sanctify and save our immortal souls.
Viva Cristo Rey! Vivat Christus Rex!
Our Lady of the Rosary, pray for us.
Saint Joseph, pray for us.
Saints Peter and Paul, pray for us.
Saint John the Baptist, pray for us.
Saint John the Evangelist, pray for us.
Saint Michael the Archangel, pray for us.
Saint Gabriel the Archangel, pray for us.
Saint Raphael the Archangel, pray for us.
Saints Joachim and Anne, pray for us.
Saints Caspar, Melchior, and Balthasar, pray for us.
Saint Margaret Cortona, pray for us.
Saint Gabriel of the Sorrowful Virgin, pray for us.
Appendix
Dr. Robert Malone Explains Why He Will Not Support Donald John Trump’s Primary Campaign
mRNA technology pioneer and prominent critic of the COVID-19 establishment Dr. Robert Malone declared that he cannot support former President Donald Trump’s bid to return to the White House as long as the candidate continues to stand by the COVID-19 vaccines his administration oversaw.
During an interview on Real America’s Voice, host David Brody asked if Trump would “acknowledge that the COVID-19 vaccines were not as safe or effective as we were told by the medical community at the time,” citing the U.S. Centers for Disease Control & Prevention’s (CDC’s) recent acknowledgment that it is investigating a potential link between the Bivalent Pfizer-BioNTech vaccine and ischemic stroke for recipients age 65 or above. (The agency later said the link was “very unlikely.”)
NEW: When asked if he has concerns about the safety of Covid Vaccines, President Trump tells me, "Well, I always do, but you have to understand. There are the pros and cons…I never demanded anybody use it. I never had a mandate. And I think that's very important to know." pic.twitter.com/P2Aic1Xezz
— David Brody (@DBrodyReports) January 17, 2023
In response, Trump launched into a self-congratulatory defense of the COVID shots, which were developed and released in a fraction of the time vaccines usually take under his administration’s Operation Warp Speed initiative. “I was able to get something approved that, you know, that has proven to have saved a lot of lives,” he said. “Some people say that I saved 100 million lives worldwide.”
“You have to understand, there are the pros and cons,” the president went on. “Some reports [say] that it’s the greatest thing that’s ever happened and we saved tens of millions of lives. Then you’ll read other reports [that] say there were some problems with the vaccine …but relatively small numbers.
“But, you know, you have many reports that say the vaccines save tens of millions of lives,” Trump reiterated. “That without the vaccines you would have had a thing … where perhaps 100 million people died.”
His answer did not sit well with Malone, who endorsed a declaration that “this will not get elected. I am out,” from Dr. Brian Tyson. He followed up by revealing that he once filmed a video meant to encourage Trump to change his mind on the subject, but it had “no impact.”
Regretfully, I stand with Brian https://t.co/wWGdfwzQcb
— Robert W Malone, MD (@RWMaloneMD) January 19, 2023
I shot a film segment designed to help DJT see the truth. No impact. As I said, it is with regret that I have to agree with Brian. This is different from Mikki’s point. This is DJT’s decision. I disagre
— Robert W Malone, MD (@RWMaloneMD) January 19, 2023
Despite the assurances of the former president and the CDC, there remains ample cause for concern about the safety of the COVID shots.
The U.S. federal government’s Vaccine Adverse Event Reporting System (VAERS) reports 33,591 deaths, 188,857 hospitalizations, 18,181 heart attacks, and 26,166 myocarditis and pericarditis cases as of January 6. An April study out of Israel indicates that COVID infection alone cannot account for such myocarditis cases, despite claims to the contrary. Jab defenders are quick to stress that reports submitted to VAERS are unconfirmed, as anyone can submit one, but CDC researchers have recognized a “high verification rate of reports of myocarditis to VAERS after mRNA-based COVID-19 vaccination,” leading to the conclusion that “under-reporting is more likely” than over-reporting.
Further, VAERS is not the only data source containing red flags. Data from the U.S. Pentagon’s Defense Medical Epidemiology Database (DMED) shows that 2021 saw drastic spikes in a variety of diagnoses for serious medical issues over the previous five-year average, including hypertension (2,181%), neurological disorders (1,048%), multiple sclerosis (680%), Guillain-Barre syndrome (551%), breast cancer, (487%), female infertility (472%), pulmonary embolism (468%), migraines (452%), ovarian dysfunction (437%), testicular cancer (369%), and tachycardia (302%).
In September, the Japanese Society for Vaccinology published a peer-reviewed study conducted by researchers from Stanford, UCLA, and the University of Maryland, which found that the “Pfizer trial exhibited a 36% higher risk of serious adverse events in the vaccine group” while the “Moderna trial exhibited a 6% higher risk of serious adverse events in the vaccine group,” for a combined “16% higher risk of serious adverse events in mRNA vaccine recipients.”
In December, Republican U.S. Sen. Ron Johnson of Wisconsin hosted a roundtable discussion during which civil rights attorney Aaron Siri detailed data from the CDC’s V-Safe reporting system revealing that 800,000 of the system’s 10 million participants, or approximately 7.7 percent, reported needing medical care after COVID injection. “Twenty-five percent of those people needed emergency care or were hospitalized, and another 48 percent sought urgent care,” Siri added. “Also, another 25 percent on top of the 7.7 percent reported being unable to work or go to school.”
Another study by a team of American, British, and Canadian researchers, published December 5 by the in the Journal of Medical Ethics, found that COVID booster mandates for university students – a relatively healthy group at relatively low risk from the virus – do far more harm than good: “per COVID-19 hospitalisation prevented, we anticipate at least 18.5 serious adverse events from mRNA vaccines, including 1.5–4.6 booster-associated myopericarditis cases in males (typically requiring hospitalisation).”
Trump’s continued support of the COVID vaccines, which are the only major item among his presidential accomplishments that has not been either reversed by the Biden administration or opposed by corporate media, is arguably the biggest liability of his 2024 campaign.
Since leaving office, he has repeatedly promoted them, including insisting that, as “one of the greatest achievements of mankind,” they would not be controversial if he were still president, and accusing his hesitant supporters of “playing right into their [the Left’s] hands,” all the while stressing that he never supported mandating them.
The persistent negative reception that message received apparently convinced Trump to drop the subject in many of his rallies, though as recently as July 2022 he complained that “we did so much in terms of therapeutics and a word that I’m not allowed to mention. But I’m still proud of that word, because we did that in nine months, and it was supposed to take five years to 12 years. Nobody else could have done it. But I’m not mentioning it in front of my people.”
Trump: But we did so much in terms of therapeutics and a word that I'm not allowed to mention. But I'm still proud of that word… We did that in nine months, and it was supposed to take five years to 12 years. But I'm not mentioning it in front of my people, pic.twitter.com/uiNoExjUmL
— Acyn (@Acyn) July 10, 2022
Trump’s presumptive main competitor for the Republican presidential nomination, Florida Gov. Ron DeSantis, initially took a similar stance of promoting the vaccines while opposing mandates, though his position markedly changed as more data became available. For more than a year, he and his administration have spoken about the ineffectiveness of the shots, and in recent months his administration has conducted its own study, which concluded that they should not be taken by young men, and pushed for a grand jury investigation into the manufacturers. (Dr. Robert Malone says he can’t support Trump while ex-president stands by COVID-19 jabs .)